2065
Relationships among cerebrovascular reactivity, grey matter volume and markers of successful aging1Concordia University, Montreal, QC, Canada, 2Biomedical Sciences, Universite de Montreal, Montreal, QC, Canada, 3Montreal Heart Institute, Montreal, QC, Canada, 4Laboratoire d'Étude de la Santé Cognitive des Ainés, Centre de recherche de l'Institut universitaire de gériatrie de Montréal, Montreal, QC, Canada, 5Kinesiology, Acadia University, Wolfville, NS, Canada, 6Medicine, Universite de Montreal, Montreal, QC, Canada, 7Montreal Neurological Institute, Montreal, QC, Canada, 8Neurology and Neurosurgery, McGill University, Montreal, QC, Canada, 9Neurology, Max Planck Institute for Human Cognitive and Brain Sciences, Leipzig, Germany, 10Cerebral Imaging Center, Douglas Mental Health University Institute- McGill University, Montreal, QC, Canada, 11Physics, Concordia University, Montreal, QC, Canada, 12PERFORM Centre, Montreal, QC, Canada
Synopsis
Aging causes decline in brain health, which has a complex relationship with fitness and cognition. Here, we aimed to disentangle the interactions between these outcomes in healthy older adults. MRI was used to acquire anatomical and cerebrovascular reactivity (CVR) in all participants. VO2max and cognitive outcomes were also tested. Results revealed that increased CVR was associated with decreased fitness and cognitive performance, whereas increased grey matter volume was associated with increased fitness. It is apparent that the relationship between brain health and fitness and cognitive outcomes is intricate and other parameters, such as cerebral blood flow, are necessary to gain further understanding.
Introduction
It is well documented that aging is associated with decreased cerebrovascular reactivity [CVR]1, cerebral blood flow [CBF]2,3, and gray matter volume [GMV]4. It is hypothesized that cerebrovascular stiffening leads to reduced CVR and CBF in aging5,6. Given that continuous and optimal blood flow is necessary for structural integrity and normal neuronal activity7, the flow reduction that occurs in aging likely leads to grey matter atrophy8 and impaired cognition9. Older adults with increased fitness levels, compared to those with lower levels, have consistently shown enhanced cognition10, however the relationship to cerebral health more ambiguous. For example, some studies have demonstrated that those with greater fitness have higher CVR when measured using Doppler ultrasound11, greater CBF12, and increased GMV13. Yet other studies demonstrate lower CVR in master athletes14, region-dependent differences in CVR1 or no difference in GMV15 using MRI. Thus, it is still unclear what the relationship between CVR and GMV is with fitness and cognitive outcomes. Given this ambiguity, we aimed to further explore these dynamic interactions. Specifically, how CVR and GMV relate to fitness levels and cognitive performance.Methods
Acquisitions were completed in 51 healthy older adults (37 females, 63 years) on a 3T MRI. An anatomical, 1mm3 MPRAGE acquisition (TR/TE/flip angle = 300ms/3ms/90°, 256x240 matrix) and a pseudo-continuous arterial spin labeling (pCASL), providing simultaneous BOLD contrast using dual-echo readouts (TR/TE1/TE2/flip angle= 2000ms/10ms/30ms/90° with 4x4x7mm voxels, 64x64 matrix and 11 slices, post-label delay=900ms, tag duration=1.5s, with a 100mm gap during a hypercapnia challenge (5mmHg end-tidal CO2 change, iso-oxic during two, 2min blocks) were collected. Participants also completed a maximal oxygen consumption (VO2 max) test, the gold standard for measuring fitness levels, and a test of executive functioning, the trail making test part B (TMTB), outside of the scanner. GM segmentation and VBM was completed using the CAT12 toolbox in SPM12. Registration was performed using ANTS16. FSL randomise GLM with threshold-free cluster enhancement (p<0.05, corrected) was used to identify if relationships existed between: i) CVR and VO2 max or TMTB; ii) GMV and VO2 max or TMTB.Results
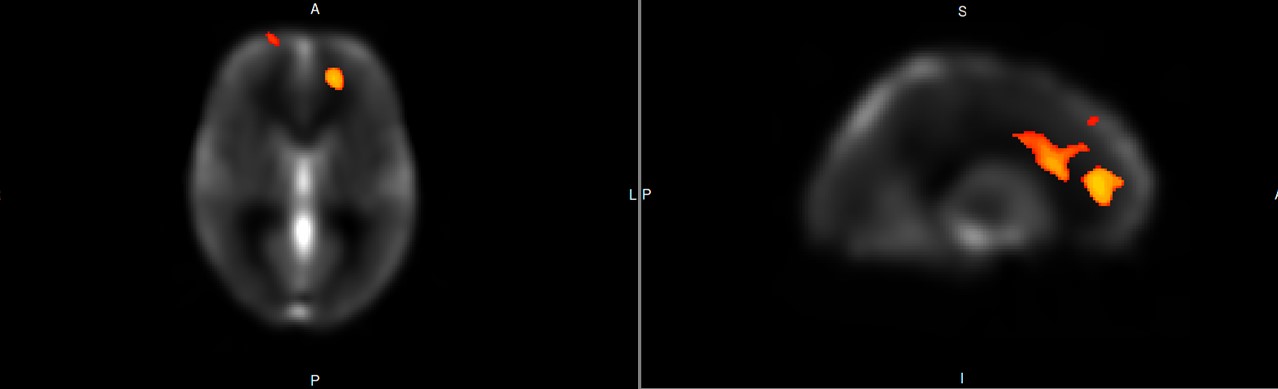
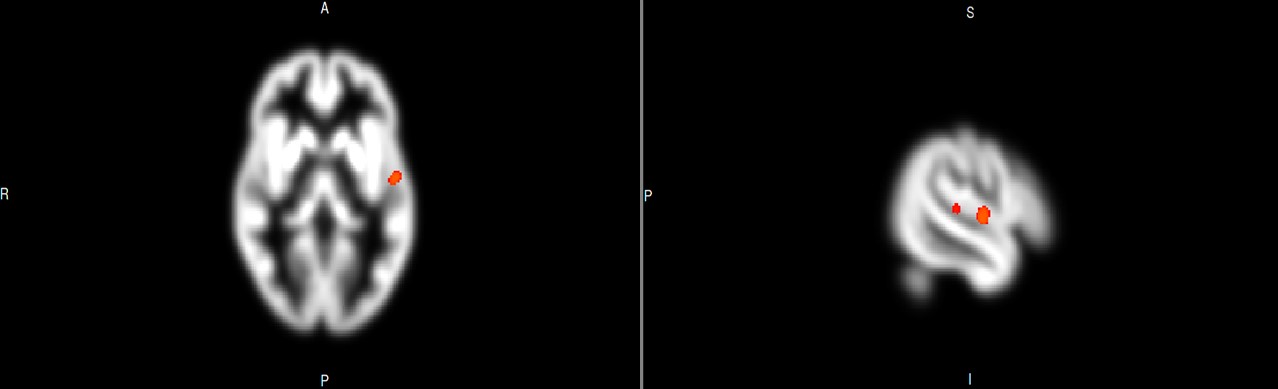
Analyses revealed significant clusters of negative relationship between CVR and VO2 max (Figure 1), and a significant positive relationship between CVR and TMTB (Figure 2), and GMV and VO2 max (Figure 3). There was no significant association between GMV and TMTB performance.Discussion
Overall, results indicate that CVR should be interpreted with caution as a marker for cerebrovascular health in healthy older adults. As previous literature has established increased VO2 max17 and decreased time to complete TMTB18 as markers of successful aging, it would be expected that increased CVR would correspond with these outcomes. Our results demonstrate that, at least in this highly healthy cohort, the opposite relationship exists. This indicates that there is a more complex interaction between CVR and brain health. However, in order to further understand this interaction and better interpret CVR, it is necessary for CBF to be included in future analyses to gain comprehensive insight. More specifically, baseline CBF and changes in CBF during hypercapnia could help disentangle the mechanisms modulating CVR, since the BOLD signal used here conflates changes in CBF baseline and reactivity. A greater baseline CBF in more fit older adults, with a similar absolute reactivity in terms of perfusion per mmHg CO2 would, for example, could lead to a seemingly lower BOLD CVR. Furthermore, a simple model was used here, and taking into account other factors such as white matter hyperintensity volume or aortic pulse wave-velocity may reveal other relationships1. Yet, it is important to highlight the positive relationship established between GMV and VO2 max, replicating not only overall findings from the literature19, but the same areas13. The lack of association between GMV and TMTB signifies that more than one domain of cognition (i.e. memory) should be included in analyses to gain a full perspective of relationships between CVR or GMV and cognitive functioning in older adults.Conclusions
Overall, these results revealed that the relationships between CVR and fitness or cognitive function have high complexity and require other markers of cerebrovascular health, such as CBF, to gain a more thorough understanding of the role CVR has in healthy older adults’ cognitive functioning. Moreover, future work should attempt to define how, CVR and GMV, together, modulate performance on VO2 max and TMTB in older adults.Acknowledgements
The authors thank Carollyn Hurst and André Cyr for their help with data acquisition, Mélanie Renaud, Cécile Madjar and Élodie Boudes for their help with logistics. They thank Jiongjiong Wang of the Department of Neurology at UCLA who provided the dual-echo pseudo-continuous arterial spin labeling sequence. This work was supported by the Canadian Institutes of Health Research (MOP 84378 and Canada Research Chair L.B.), the Canada Foundation for Innovation (Leaders Opportunity Fund 17380), the Ministère du développement économique, de l’innovation et de l’exportation (PSR-SIIRI-239), the Canadian National Sciences and Engineering Research Council (R0018142, RGPIN-2015-04665) and the Heart and Stroke Foundation of Canada (N.I.A. C.J.G.)References
1. Gauthier CJ, Lefort M, Mekary S, et al. Hearts and minds: linking vascular rigidity and aerobic fitness with cognitive aging. Neurbiol Aging. 2014; 36 (1): 304-14
2. Pantano P, Baron JC, Lebrun-Grandie P, et al. Regional cerebral blood flow and oxygen consumption in human aging. Stroke. 1984; 15(4): 635-41
3. Martin AJ, Friston KJ, Colebatch JG and Frackowiak RS. Decreases in regional cerebral blood flow with normal aging. J Cereb Blood Flow Metab.1991; 11: 684-9
4. DeCarli C, Massaro J, Harvey D, et al. Measures of brain morphology and infarction in the framingham heart study : establishing what is normal. Neurobiol of Aging. 2005; 26(4): 491-510
5. Fluck D, Beaudin AE, Steinback CD, et al. Effects of aging on the association between cerebrovascular responses to visual stimulation, hypercapnia and arterial stiffness. Front Physiol. 2014; 5(49)
6. Gauthier CJ, Madjar C, Desjardins-Crepeau L, et al. Age dependence of hemodynamic response characteristics in human functional magnetic resonance imaging. Neurobiol Aging. 2013; 34(5):1469-85
7. Erecinska M and Silver IA. ATP and brain function. J Cereb Blood Flow Metab. 1989; 9: 2-19
8. de la Torre JC. Cerebral hemodynamics and vascular risk factors: setting the stage for Alzheimer’s disease. J Alzheimers Dis. 2012; 32(3): 553-67
9. Ogoh S. Relationship between cognitive function and regulation of cerebral blood flow. J Physiol Sci. 2017; 67: 345-51
10. Wendell CR, Gunstad J, Waldstein SR, et al.Cardiorespiratory fitness and accelerated cognitive decline with aging. J Gerontol A Biol Sci Med Sci. 2014; 69(4): 455-62
11.Barnes JN, Taylor JL, Kluck BN, Johnson CP and Joyner MJ. Cerebrovascular reactivity is associated with maximal aerobic capacity in healthy older adults. J Appl Physiol, 2013; 114: 1383-7
12. Zimmerman B, Sutton BP, Low KA, et al. Cardiorespiratory fitness mediates the effects of aging on cerebral blood flow. Front Aging Neurosci. 2014; 6(59)
13. Colcombe S and Kramer AF. Fitness effects on the cognitive function of older adults: a meta-analytic study. Psychol Sci. 2003; 14:125-30Thomas BP, Yezhuvath US, Tseng BY, et al. Life-long aerobic exercise preserved baseline cerebral blood flow but reduced vascular reactivity to CO2. J Magn Reson Imaging. 2013; 38: 1177-83
14. Freudenberger P, Petrovic K, Sen A, et al. Fitness and cognition in the elderly. The austrian stroke prevention study. Neurology. 2016; 86:418-24
15. Avants BB, Epstein CL, Grossman M and Gee JC. Symmetric diffeomorphic image registration with cross-correlation: evaluating automated labeling of elderly and neurodegenerative brain. Med Image Anal. 2008; 12(1): 26-41
16. Thielke S and Diehr P. Transitions among health states using 12 measures of successful aging in men and women: results from the cardiovascular health study. J Aging Res. 2012; article ID: 243263
17. Fabbri E, An Y, Zoli M, Tanaka T, et al. Association between accelerated multimorbidity and age-related cognitive decline in older baltimore longitudinal study of aging participants with dementia. J Am Geriatr Soc. 2016; 64(5): 965-72
18. Ahlskog JE, Geda YE, Graff-Radford NR and Petersen RC. Physical exercise as a preventative or disease-modifying treatment of dementia and brain aging. Mayo Clin Proc. 2011; 86(9): 876-84
Figures