2064
Retinal Vascular Fractal Dimension and Cerebral Blood Flow, a pilot study1Department of Ophthalmology, Nîmes University Hospital, Nimes, France, 2Gui de Chauliac Hospital, I2FH, Institut d'Imagerie Fonctionnelle Humaine, Montpellier, France, 3Neuroradiology, I2FH - CHU Gui de Chauliac, Montpellier, France, 4U1061, INSERM, Montpellier, France, 5Department of Ophthalmology, Gui De Chauliac Hospital, Montpellier, France
Synopsis
The retinal vascular fractal dimension (FD) is a marker of retinal vascular complexity of the vascular tree. It has been associated with systemic disorders but also with neurodegenerative and cerebrovascular diseases. The purpose of this study was to explore the relationship between cerebral blood flow (CBF), retinal vascular FD and other retinal vascular markers. CBF was estimated in vascular territories using 2D PASL sequence. CBF was positively associated to venular FD (R2=0.32, p=0.03). Non-invasive exploration of the retinal vasculature may be used as a proxy measure, with the condition of retinal vessels possibly reflecting the condition of the cerebral vasculature.
INTRODUCTION
Ocular and brain microcirculation share embryological and histological similarities. The retinal vascular fractal dimension (FD) is a marker of retinal vascular complexity of the vascular tree. It has been associated with systemic disorders but also with neurodegenerative and cerebrovascular diseases. Arterial spin labeling (ASL) is a non-invasive technique to evaluate cerebral blood flow (CBF). The purpose of this study was to explore the relationship between CBF, retinal vascular FD and other retinal vascular markers.METHODS
Cross-sectional analysis comprising 26 individuals ≥ 65 years old from the Cognitive REServe and Clinical ENDOphenotype (CRESCENDO) cohort of healthy older adults. Retinal vascular FD was measured from fundus photographs by using the semi-automated Singapore Eye Vessel Assessment (SIVA) software1. SIVA automatically identifies the optic disc, places a grid with reference to the center of optic disc, identifies the vessel type and calculates retinal parameters in a zone of 0.5 to 1.0 disc diameter away from the optic disc margin. The FD was calculated from a skeletonized line tracing by using the box-counting method, which divides each image into a series of squares for various side lengths2. An example of high and low FD is presented in the figure 1.
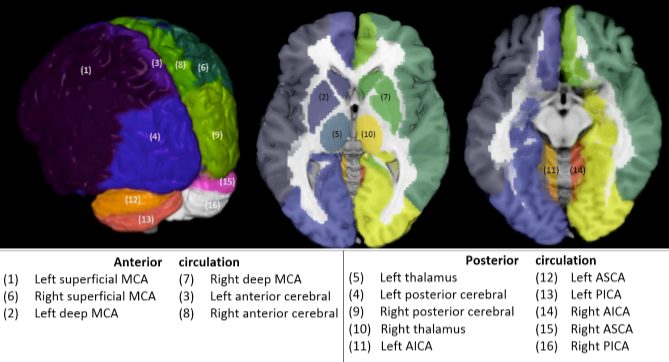
Neuroimaging data were collected by using a 3T magnet system (Skyra, Siemens, Germany) with a 32-channel head coil. Structural images (3DT1) were acquired with the parameters field of view=25 x 25 cm, TE=2.5 ms, TR=1690 ms, flip angle=9°, voxel size=0.98 x 0.98 x 1 mm3, 176 slices. Fluid-attenuated inversion recovery (FLAIR) images were acquired to estimate white-matter (WM) lesions with the parameters field of view=22 x 22 cm, TE=111 ms, TR=7000 ms, flip angle=150 °, voxel size=0.86 x 0.86 x 3 mm3, 39 slices. CBF data were acquired by using a 2-D pulsed ASL sequence, PICORE-Q2TIPS, with TI1/TI2/TR/TE=700/2000/3000/20 ms, 52 repetitions, 16 slices, and voxel size=3.44x3.44x6 mm3. To ensure a correct estimation of the CBF, partial volume effects correction3 was applied in native space, with a 7x7x1 voxel regression kernel. CBF computation involved a one-compartment model4. CBF was extracted for each vascular territory (Figure 2) .
We analyzed the association between regional CBF and the following retinal vascular features: total, arterial and venous FD; CRAE, CRVE; arteriole and venule curvate tortuosity; and arteriole and venule branching angle. To assess the trend of CBF changes with respect to retinal vascular variables, one linear regression model was created and adjusted for sex and age. Bonferroni’s correction was used in all pairwise comparisons.
RESULTS
CBF was positively associated with venular FD (R2=0.32, p=0.03) after adjustment for age and sexe (Table 1). This association was driven by a higher association between venular FD in the anterior versus posterior CBF (R2=0.001 [p=0.35] vs. R2=0.16 [p=0.007], respectively). Global CBF was correlated with arteriolar branching angle (R2=0.23, p=0.01) and tortuosity (R2=0.20, p=0.02). Global CBF was not correlated with other SIVA parameters: arteriolar FD (R2=0.02, p=0.48), central retinal arteriolar equivalent (R2=0.02, p=0.41), central retinal venular equivalent (R2=0.01, p=0.51), venous tortuosity (R2=0.12, p=0.09), or venular branching angle (R2 =0.07, p=0.19).DISCUSSION
Our results suggest a positive correlation between retinal FD and CBF, a stronger association observed with venular FD in anterior CBF. Arteriolar branching angle and arterial tortuosity were associated with CBF.
The association we observed between retinal FD and anterior (rather than posterior) CBF may be related to a common vascular origin from the internal carotid artery. The posterior CBF is from the basilar trunk, which is not related to the retinal microcirculation5. Cardiovascular risk factors and the subsequent arteriosclerosis decrease CBF6. Non-invasive and easy exploration of the retinal vasculature may be used as a proxy measure, with the condition of retinal vessels possibly reflecting the condition of the cerebral vasculature.
Most previous studies analyzed the association between total retinal vascular FD and cerebrovascular diseases but did not distinguish arterial and venular FD. In this study, we found CBF associated more with venular than arteriolar FD. Venular FD could be the retinal factor most associated with cerebral dysfunction. This finding is consistent with the study of Williams et al.7, who found lower venular FD in Alzheimer disease, which is also influenced by cardiovascular risk factors. In contrast, the association between arteriolar FD and Alzheimer disease did not persist in their models7.
CONCLUSION
This pilot study suggests retinal complexity summarized by the FD was the main variable associated with cerebral perfusion. It may be evaluated in larger prospective clinical studies for early and non-invasive detection of subclinical cerebrovascular pathologies including dementia and stroke.Acknowledgements
No acknowledgement found.References
1. Lau, Q., Li Lee, M., Hsu, W. & Wong, T. The Singapore Eye Vessel Assessment System. in Image Analysis and Modeling in Ophthalmology 143–160 (CRC Press, 2014).
2. Mainster, M. A. The fractal properties of retinal vessels: embryological and clinical implications. Eye Lond. Engl. 4 ( Pt 1), 235–241 (1990).
3. Bruening, D. E., Dharssi, S., Lazar, R. M., Marshall, R. S. & Asllani, I. Improved partial volume correction method for detecting brain activation in disease using Arterial Spin Labeling (ASL) fMRI. Conf. Proc. Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. IEEE Eng. Med. Biol. Soc. Annu. Conf. 2015, 5441–5444 (2015).
4. Wang, J. et al. Pediatric perfusion imaging using pulsed arterial spin labeling. J. Magn. Reson. Imaging JMRI 18, 404–413 (2003).
5. Rai, A. T., Rodgers, D., Williams, E. A. & Hogg, J. P. Dimensions of the posterior cerebral circulation: an analysis based on advanced non-invasive imaging. J. Neurointerventional Surg. 5, 597–600 (2013).
6. Pase, M. P., Grima, N. A., Stough, C. K., Scholey, A. & Pipingas, A. Cardiovascular disease risk and cerebral blood flow velocity. Stroke 43, 2803–2805 (2012).
7. Williams, M. A. et al. Retinal microvascular network attenuation in Alzheimer’s disease. Alzheimers Dement. Amst. Neth. 1, 229–235 (2015).
Figures
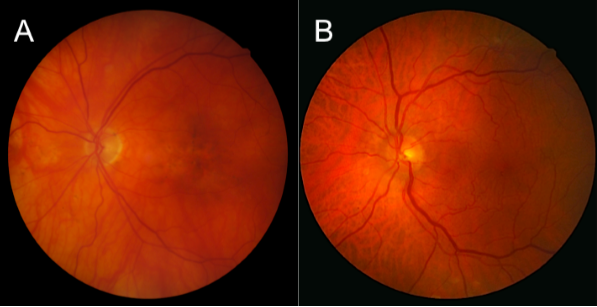
Figure 1. Retinal photographs for fractal dimension (FD). (A) Low retinal vascular FD: total vascular FD=1.37. (B) High FD: total vascular FD= 1.49.