1966
Diffusion-prepared magnetic resonance neurography for the visualization of the Facial nerve1Radiology, The Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital, Amsterdam, Netherlands, 2Head and Neck Oncology and Surgery, The Netherlands Cancer Institute - Antoni van Leeuwenhoek Hospital, Amsterdam, Netherlands, 3Oral and Maxillofacial Surgery, Academic Medical Center, Amsterdam, Netherlands, 4Radiology, Leiden University Medical Center, Leiden, Netherlands
Synopsis
The aim of the study was to investigate the feasibility of Diffusion-prepared MRI (D-prep MRI) to visualize the Facial nerve in head and neck cancer patients. Twenty-four patients (12 male, 60±11 year) received a D-prep MRI, where the main trunk and branches of the Facial nerve is reviewed by one neuro/head and neck radiologists. The main trunk was visible in fifteen patients and in four, six, six and one patients for the posterior auricular, zygomaticofacial, cervicofacial and temporal branches respectively. D-prep MRI is able to visualize the Facial nerve in most cases, but further improvement is required.
Purpose: Facial nerve damage can be a serious complication of parotid surgery. Pre- or peroperative localization of the Facial nerve may help the surgeon to avoid this complication. Nowadays, conventional MRI techniques are limited to visualize the course of this nerve. Diffusion-prepared MRI (D-prep MRI) is a novel technique designed to specifically visualize nerve structures1,2, what can provide added value to the surgeon. This study evaluates the ability and extent D-prep MRI to detect the Facial nerve.
Methods: Patients: D-prep MRI was performed in 24 patients (13 male/11 female, mean age 60±11 years) that underwent a 3 Tesla MRI (Philips, Best, The Netherlands) for (suspected) head and neck cancer between December 2016 and August 2017.
MR protocol: The D-prep sequence is based on published protocols1,2, with a T2-contrast based preparation pulse and a 3D tissue-specific variable refocusing flip-angle rapid acquisition with relaxation enhancement (RARE) readout. The patients were sagittal oriented scanned in an twenty-two-channel head and neck coil, with a field of view (FOV) including the healthy behalf of the face from neck level II, III and V. Other imaging parameters are a flip angle (FA) of 90º, voxel size of 0.5 x 0.5 x 1.0 mm3, repetition time (TR) of 2500 ms and echo time (TE) of 180 ms. Fat is suppressed using a spatially adiabatic inversion recovery (SPAIR). The average scan duration is 2 min 30 s.
Data analysis: The visibility, length and thickness of the different branches of the Facial nerve were assessed by one neuro/head and neck radiologist based on the course of the nerve. The main trunk was defined as the course from the foramen stylomastoideum to the bifurcation of the zygomaticofacial and cervicofacial.
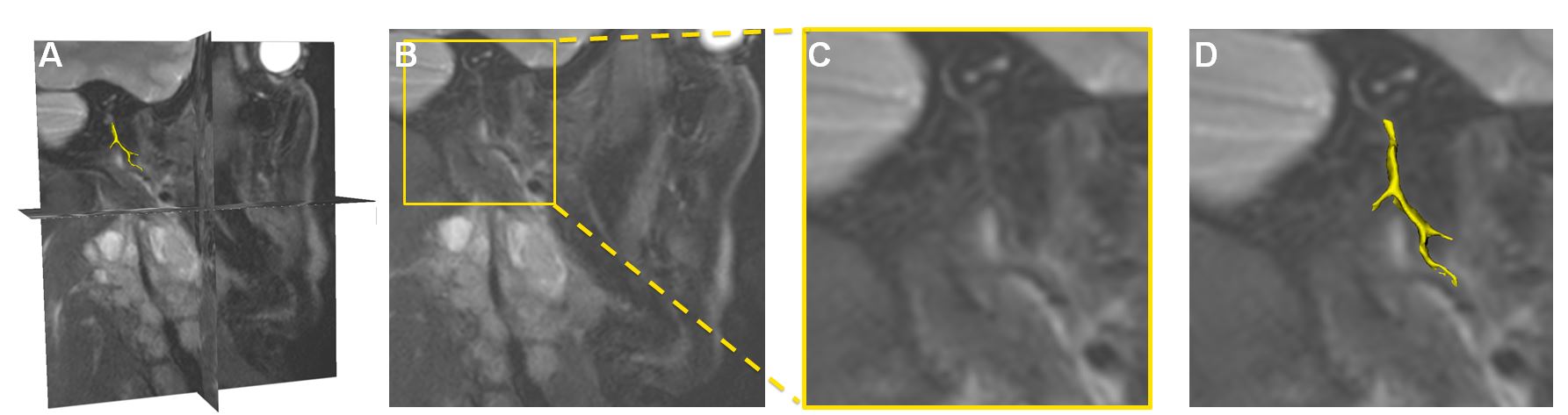
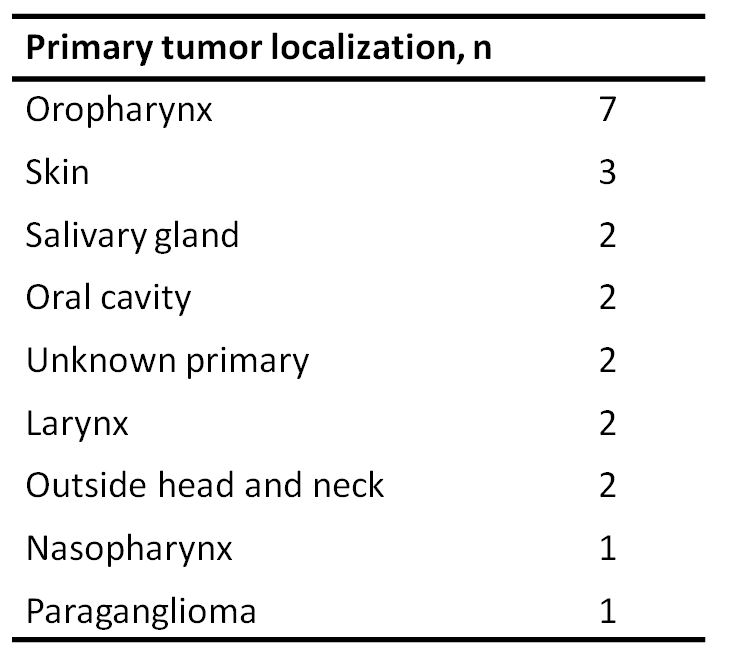
Results: Two patients were excluded because of poor MRI quality. For the remaining 22 patients, the primary tumor localization is summarized in Table 1. In these patients the main trunk was visible in 15 patients, with a length between 4 and 26 mm and a median thickness of 1.3 mm. The posterior auricular nerve was visible in 4 patients (6 – 11 mm; 0.9 mm), the zygomaticofacial branch in 6 patients (2 – 12 mm; 1.1 mm), the cervicofacial branch in 6 patients (1 – 23 mm; 1.0 mm) and the temporal in 1 patient (6 mm; 1.6 mm). In 7 patients, the Facial nerve was not assessable because of movement artefacts of the D-prep or low fat content of the parotic gland. Figure 1 visualized an example of the D-prep MRI of a patient.
Discussion: The low fat content of the parotic gland might disturb the visibility of the Facial nerve. The D-prep MRI is based on fat-suppression, which might not be optimal in these cases. Other MR parameters might also influence the results, such as the fold-over suppression, shimming and the flow suppression. In some cases, small arteries with low flow velocity are visible as a result of the lacking flow suppression. Besides this, the dimensions of the main trunk and branches of the Facial nerves are limited to measuring bias, only one observer and the voxel size. Furthermore, only one half of the human face is in the FOV because of limited scanning time.
Conclusion: The Facial nerve can be identified and its course delineated with D-prep MRI in most cases. Further optimization of this sequence will hopefully result in more detailed visualization and delineation of the Facial nerve branches. Further research will be focussed on the association between D-prep MRI and the surgical findings during surgery to introduce this new sequence in the clinical workflow for better informing patients preoperative.
Acknowledgements
No acknowledgement found.References
1. Yoneyama M, Takahara T, Kwee T.C, et al. Rapid High Resolution MR Neurography with a Diffusion-weighted Pre-pulse. Magn Reson Med Sci. 2013;12(2): 111-119.
2. Buckle T, KleinJan G.H, Engelen T, et al. Diffusion-weighted-preparation (D-prep) MRI as a future extension of SPECT/CT based surgical planning for sentinel node procedures in the head and neck area? Oral Oncol. 2016:60:48-54
Figures