1964
The feasibility of ultrashort echo time imaging for visualization of sinonasal and skull base bony structures: preliminary study1Ajou Univeristy Medical Center, Suwon, Republic of Korea, 2GE healthcare, Seoul, Republic of Korea
Synopsis
We evaluate the feasibility of ultrashort echo time (UTE) imaging in the visualization of sinonasal and skull base bony structures. MRI with UTE imaging are feasible to assess not only the normal bony structures but also diverse anatomic variations of sinonasal cavity and skull base without radiation exposure. This technique may lead to a new application of diagnostic MRI in head and neck imaging and could be expected to prevent additional CT imaging and consequently reduce radiation exposure.
INTRODUCTION
The CT is essential imaging modality for evaluation of sinonasal and skull base structures. However, the general concerns for radiation exposure from the CT scan have been raised and the sinonasal CT includes lenses and salivary glands which are especially sensitive to radiation1. On the other hand, the MRI is free to radiation exposure but it has been unable to visualize bony structures due to the extremely short T2 of the compact bone. Ultrashort echo time (UTE) imaging is an MRI method that allows for direct visualization of tissues with very short T2 and it has been used to evaluate bones and other connective tissues2, 3. Recent reports evaluated the middle ear ossicles using UTE sequence in head and neck area4, 5. The aim of this study was to evaluate the feasibility of ultrashort echo time (UTE) imaging in the visualization of normal sinonasal and skull base bony structuresMETHODS
In this retrospective study, 15 patients (median age: 51 [20-83], 6 females, 9 males) who underwent MRI including UTE sequence and had previous head CT images that reconstructed as 1mm thickness using bone algorithm and acquired within interval of 6 months were included. UTE imaging was acquired with following parameters: TR 6.4 ms, TE 0.032 ms, flip angle 2˚, 0.8x0.8x0.8mm resolution, FOV 200x200, matrix 320x320, 6 min 25 s acquisition time. Two independent reviewers evaluated the visualization of 19 notable anatomical landmarks6 and two anatomical variation types (Keros type and uncinate process attachment type). The visibility of anatomic landmarks were scored as 3 scales as follows; 0= not demonstrated, 1= demonstrated but not clearly visualized, 2 = clearly visualized. In addition, radiologist’s subjective impression for the overall diagnostic imaging quality was recorded as 5 point scales. The inter-reader and inter-modality agreements were estimated.RESULTS
The average image quality scores for visibility of 19 anatomic landmarks are 1.86 ± 0.12. Only 7 structures in 3 patients were not demonstrated in UTE images (1.3% of all structures evaluated in study population). The inter-reader agreement for visualization of anatomic landmarks were distributed from 56.7 % to 100 % of concordance. The inter-reader agreements for assessing anatomic variations, the uncinate process attachment type and the Keros type, were moderate (weighted k=0.52) to good (weighted k=0.79), consequently. Compared to CT scan, the inter-modality agreements were good (weighted k=0. 62) to the perfect (weighted k=1.00), consequently. The overall diagnostic quality were scored from 2 to 5 (mean 3.93± 0.12) with good inter-reader agreement (weighted k=0.66).DISCUSSION
To our knowledge, this is first study of MR visualization of the sinonasal and skull base bony structures. The sinonasal disorders are characterized by repetitive imagings due to postoperative recurrence and high prevalence in children. Although the diagnostic value of MRI is limited by the susceptibility artifact from air in sinonasal cavity, the MRI with UTE could be helpful in case of patients needing repeated CT scans and pediatrics to reduce radiation exposure.CONCLUSION
With UTE imaging, MRI applications for sinonasal and skull base bony structures are feasible. This technique may lead to a new application of diagnostic MRI on head and neck imaging.Acknowledgements
No acknowledgement found.References
1. Toohey RE1. Meeting the Needs of the Nation for Radiation Protection: Summary of the 52nd Annual Meeting of the National Council on Radiation Protection and Measurements. Health Phys. 2017 Feb;112(2):230-234
2. Tyler DJ, Robson MD, Henkelman RM, Young IR, Bydder GM. Magnetic resonance imaging with ultrashort TE (UTE) PULSE sequences: technical considerations. J Magn Reson Imaging. 2007 Feb;25(2):279-89.
3. Holmes JE, Bydder GM. MR imaging with ultrashort TE (UTE) pulse sequences: Basic principles. Radiography. 2005;11:163-74
4. Naganawa S, Nakane T, Kawai H, Taoka T, Suzuki K, Iwano S, Satake H, Grodzki D. Visualization of Middle Ear Ossicles in Elder Subjects with Ultra-short Echo Time MR Imaging. Magn Reson Med Sci. 2017 Apr 10;16(2):93-97
5. Yamashita K, Yoshiura T, Hiwatashi A, Kamano H, Honda H. Ultrashort echo time imaging of normal middle ear ossicles: a feasibility study. Dentomaxillofac Radiol. 2012 Oct;41 (7):601-4
6. Demeslay J, Vergez S, Serrano E, Chaynes P, Cantet P, Chaput B, de Bonnecaze G. Morphological concordance between CBCT and MDCT: a paranasal sinus-imaging anatomical study. Surg Radiol Anat. 2016 Jan;38(1):71-8
Figures
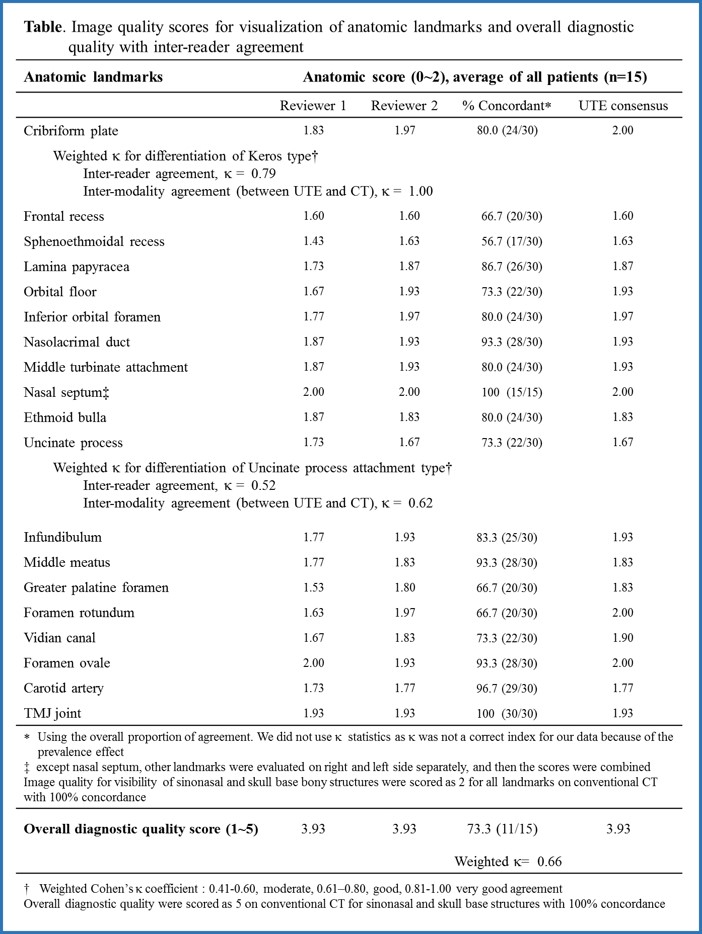

Figure. Comparison of UTE and CT images for sinonasal and skull base bony structures. (a) Skull base foramens, Foramen rotundums (arrows) and vidian canals (arrowheads) are well visualized on UTE (b) The uncinated process attachment type, uncinated process of right side attach to the roof of the ethmoid and that of left side attach to the lamina papyracea, are well documented on UTE (c) Keros type for olfactory fossa, depth of olfactory recess are less than 7mm (bar on image) at both side, they are classified as Keros type 2.