1956
Imaging and involvement of visual pathways in children undergoing epilepsy surgery1Developmental Imaging and Biophysics Section, UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 2Neurosurgery, UCL Great Ormond Street Institute of Child Health, London, United Kingdom, 3Department of Clinical and Experimental Epilepsy, UCL Institute of Neurology, London, United Kingdom, 4Ophthalmology, UCL Great Ormond Street Institute of Child Health, London, United Kingdom
Synopsis
Surgery is a key approach for achieving seizure control in children with epilepsy but it can affect or be in the vicinity of the optic radiations. Whilst tractography has shown that damage to optic radiations leads to postoperative visual field defects in adults it has not yet been properly explored in children. In this study we successfully performed tractography reconstructions in a paediatric cohort undergoing surgery. Furthermore, we showed that in cases with pre- and post-surgical visual function assessment, involvement of optic radiations corresponded to visual function disturbances. This highlights the importance of tractography to aid pre-surgical evaluation in children.
Introduction
Surgery is a key approach for achieving seizure control in children with refractory focal epilepsy. In adults the most common type of focal epilepsy is temporal lobe epilepsy (TLE), and the most common surgical approach is anterior temporal lobe resection (ATLR)[1]. TLE represents a smaller proportion of focal epilepsy in children however, where there is a wider range of epilepsy conditions and syndromes. Associated surgeries in these cases could affect or be in the vicinity of the optic radiations, potentially disturbing visual function. Tractography has played a key role in demonstrating damage to the optic radiation leading to postoperative visual field defects in adults[2], but its involvement is not yet properly explored in paediatric cohorts[3][4]. Here, we use tractography to determine optic radiation involvement in a paediatric series, by investigating whether pre-surgical reconstructions of the optic radiations overlap with the resection margin as measured using standard anatomical post-surgical T1-weighted MRI.Methods
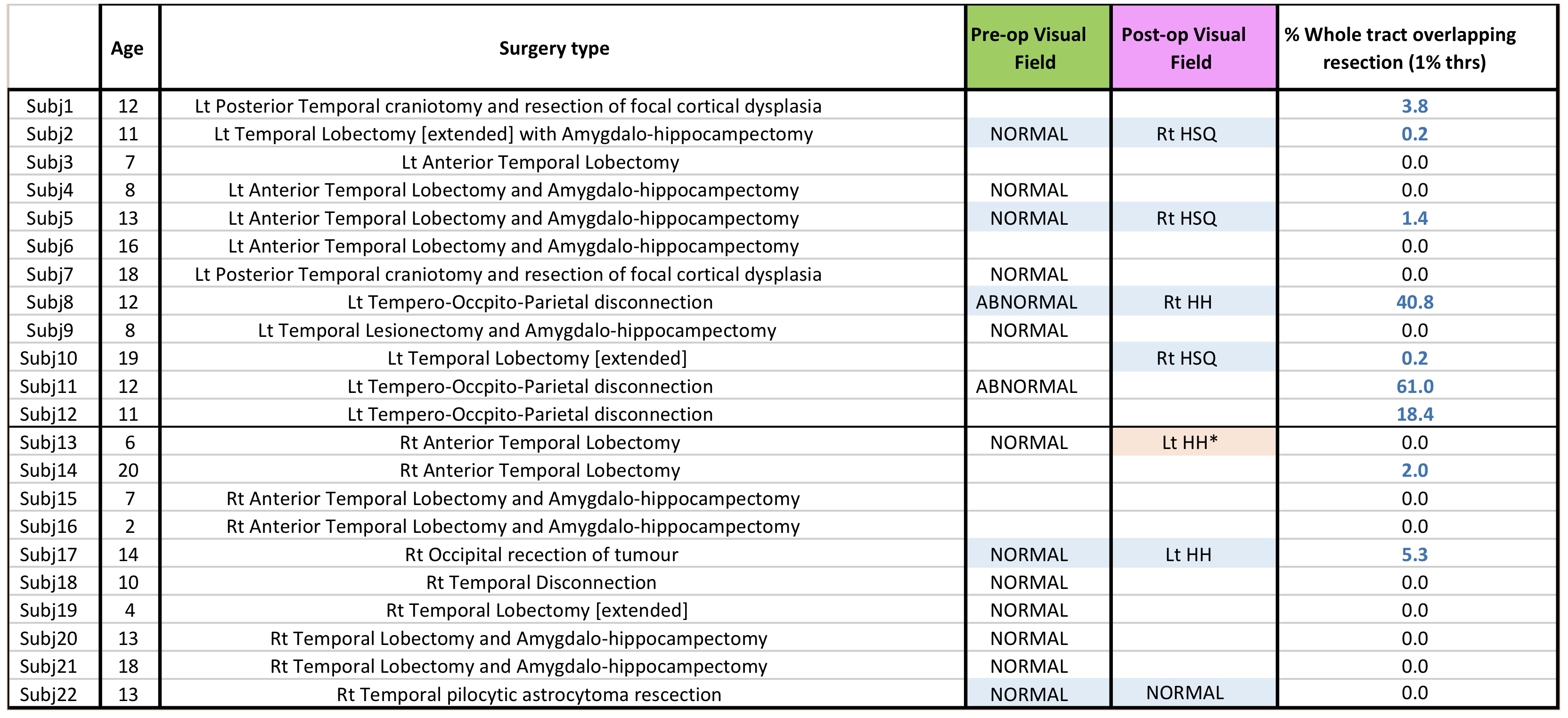
Data inclusion criteria:Patients with parietal, temporal and occipital resections were included in this study (Table 1) in a retrospective manner (n=22).
Data acquisition:Each patient underwent a two shell dMRI protocol on a Siemens Prisma 3.0T clinical system (Siemens Healthcare, Erlangen, Germany). Data were collected using a multi-band diffusion weighted single-shot spin echo EPI, with an acceleration factor of 2; images were acquired for two sets of 60 non-collinear directions, using a weighting factor of 1000s.mm-2 and 2200s.mm-2 respectively, along with 13 additional T2-weighted (b = 0) volumes. 66 axial slices of thickness 2.0mm were imaged, using a FOV=220×220mm and 110×110 voxel acquisition matrix, for a final image resolution of 2.0×2.0×2.0mm; TE=60ms and TR=3050ms. In addition, a T1-weighted 3D FLASH structural image was acquired using 176 contiguous sagittal slices, FOV=256×240mm and 1×1×1mm image resolution; TE=4.9ms and TR=11ms. Imaging data was acquired before and after surgery. Additionally, visual field function was evaluated with Goldmann perimetry (Table 1).
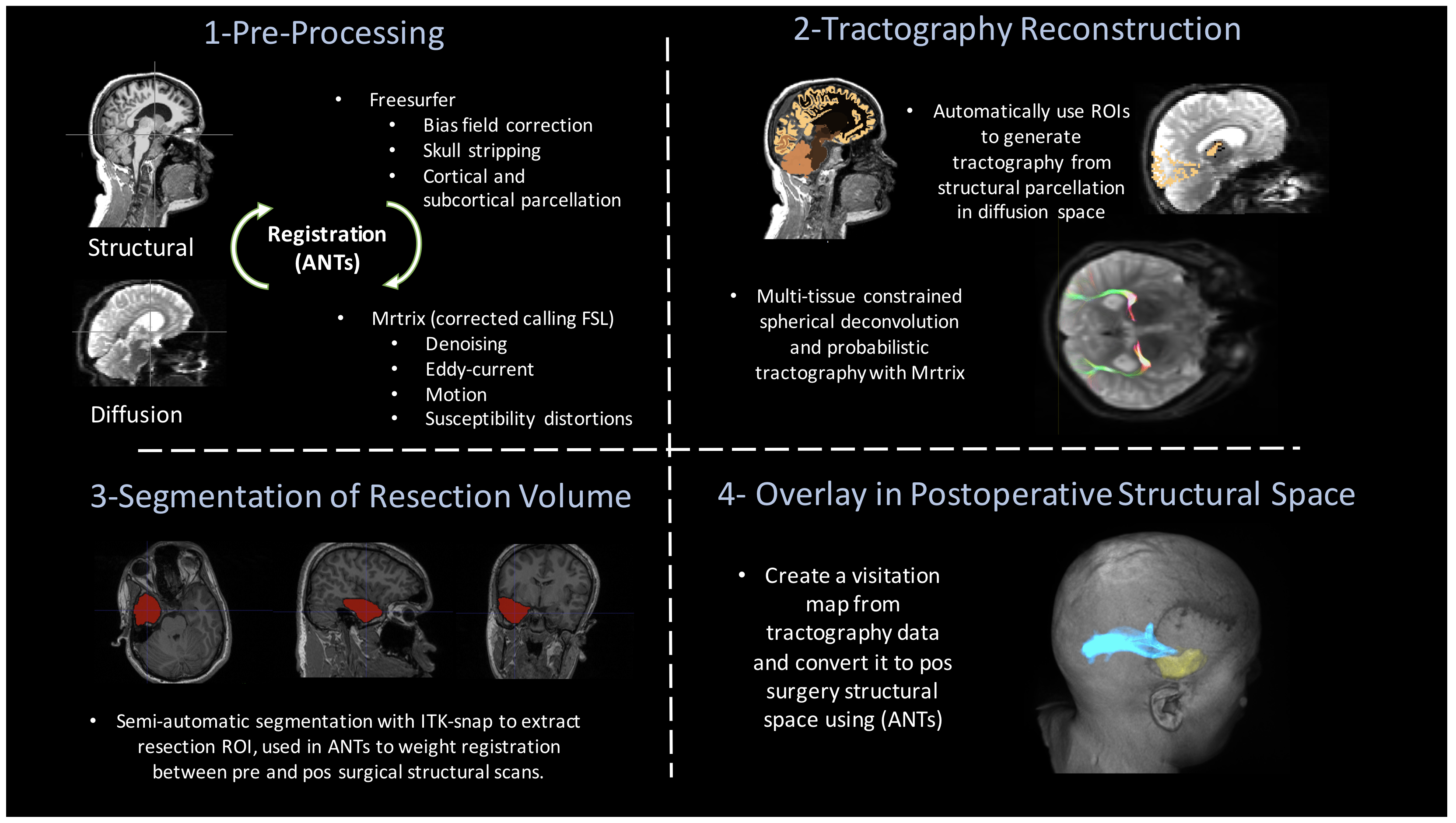
Data Processing:dMRI data were denoised using MRtrix’s[6] implementation of the method developed by Veraart[5]. Furthermore, TOPUP and EDDY were used to correct for susceptibility distortions and to perform motion and eddy current correction[7]. Freesurfer[8] was applied to pre-surgical structural images and the generated parcellations registered to diffusion space using the ANTs software[9]. Additionally, semi-automatic segmentation of the resected volume was performed with ITK-snap. After pre-processing, dMRI data was used in MRtrix CSD pipeline, estimating both a multi-tissue response function and fibre orientation distribution fields. These were then used for probabilistic tractography (iFOD2 algorithm), with an angular threshold of 90°, and selected number of streamlines of 5000. Particularly, the posterior part of the thalamus was used as seed region, and a composite occipital region (lateral occipital, lingual and pericalcarine cortex) used as include region. A CSF and a contra-lateral hemispheric mask were also used as excluding regions. Lastly, a map depicting the probability of anatomical connections was derived from the reconstructed optic radiations. These were then registered to post-surgical space, and the overlap with the resection margin quantified.
Results and Discussion
In 9/22 children there was overlap between the pre-surgical optic radiation tractography and post-surgical resection margin on T1-weighted MRI. To quantify this overlap, the probability of connection maps were thresholded at 1% and the number of voxels in common with the resection area presented as a fraction of the whole map (Table 1). Where visual field data was available before and after surgery the presence of overlap corresponded to abnormal post-surgical visual function following normal pre-surgical visual function for subjects 2, 5, 8 and 17. Subject 8 showed a complete loss of right visual field, despite having a pre-existing visual deficit, which is compatible with the high overlap found. Subject 22 had no pre-existing or post-surgical deficits and accordingly no corresponding overlap of the optic radiations with the resection margin was found. Although there was a report of a left Homonymous hemianopia for Subject 13, no overlap was found.Conclusion
In this study we successfully performed tractography reconstructions of the optic radiations in a paediatric cohort undergoing epilepsy surgery. Furthremore, we were able to evaluate the overlap of pre-surgical reconstructions with the resected area after surgery. The optic radiations were involved in the resection margin in 40% of cases. This first report in a peadiatric series highlights the relevance and importance of optic radiation tractography for future pre-surgical evaluation in children undergoing epilepsy surgery. In 5/6 cases with pre- and post-surgical visual function assessment, involvement of the optic radiations corresponded to subsequent disturbance of visual function. Future work will focus on relating the nature and degree of visual disturbance to optic radiation involvement in the resection margin.Acknowledgements
This research/study/project was funded by Fight for Sight and supported by the National Institute for Health Research Biomedical Research Centre at Great Ormond Street Hospital for Children NHS Foundation Trust and University College London. GOSH BRC. G.Winston additionally acknowledges MRC (MR/M00841X/1).References
[1] R. J. Piper, M. M. Yoong, J. Kandasamy, and R. F. Chin, “Application of diffusion tensor imaging and tractography of the optic radiation in anterior temporal lobe resection for epilepsy: A systematic review,” Clinical Neurology and Neurosurgery, vol. 124, pp. 59–65, Sep. 2014.
[2] G. P. Winston, P. Daga, M. J. White, C. Micallef, A. Miserocchi, L. Mancini, M. Modat, J. Stretton, M. K. Sidhu, M. R. Symms, D. J. Lythgoe, J. Thornton, T. A. Yousry, S. Ourselin, J. S. Duncan, and A. W. McEvoy, “Preventing visual field deficits from neurosurgery.,” Neurology, vol. 83, no. 7, pp. 604–611, Aug. 2014.
[3] M. Dayan, M. Munoz, S. Jentschke, M. J. Chadwick, J. M. Cooper, K. Riney, F. Vargha-Khadem, and C. A. Clark, “Optic radiation structure and anatomy in the normally developing brain determined using diffusion MRI and tractography,” Brain Structure and Function, vol. 220, no. 1, pp. 291–306, Oct. 2013.
[4] A. Liava, R. Mai, L. Tassi, M. Cossu, I. Sartori, L. Nobili, G. Lo Russo, and S. Francione, “Paediatric epilepsy surgery in the posterior cortex: a study of 62 cases.,” Epileptic Disord, vol. 16, no. 2, pp. 141–164, Jun. 2014.
[5] J. Veraart, D. S. Novikov, D. Christiaens, B. Ades-Aron, J. Sijbers, and E. Fieremans, “Denoising of diffusion MRI using random matrix theory.,” NeuroImage, vol. 142, pp. 394–406, Nov. 2016.
[6] J.-D. Tournier, F. Calamante, and A. Connelly, “MRtrix: Diffusion tractography in crossing fiber regions,” Int. J. Imaging Syst. Technol., vol. 22, no. 1, pp. 53–66, Feb. 2012.
[7] J. L. R. Andersson and S. N. Sotiropoulos, “An integrated approach to correction for off-resonance effects and subject movement in diffusion MR imaging.,” NeuroImage, vol. 125, pp. 1063–1078, Jan. 2016.
[8] B. Fischl, “FreeSurfer,” NeuroImage, pp. 1–8, Feb. 2012.
[9] B. B. Avants, N. J. Tustison, M. Stauffer, G. Song, B. Wu, and J. C. Gee, “The Insight ToolKit image registration framework.,” Front. Neuroinform., vol. 8, no. 52, p. 44, 2014.
Figures