1937
The fronto-parietal connectivity in freezing of gait: a left/right imbalance ?1Neurology Department, Lille University Hospital Center, Lille, France, 2Lille University Hospital Center, Lille, France, 3Radiology Department, Lille University Hospital Center, Lille, France
Synopsis
The multimodal MRI assessment is here used to better understand the previous known parietoprefrontal networks' abnormalities in parkinsonian patients with freezing of gait. Anatomic disconnection was observed in the right prefrontal cortex in those patients and functional disconnection was major from the left one. The imbalance between left and right networks is discussed heyard the pathophysiology of freezing.
Background
Freezing of gait in Parkinson's disease is a paroxysmal gait dysfunction, marked by the absence of the forward progression of the foot, despite the intention to walk, with a high risk of fall [1]. Concerning its pathophysiology, it seems to result from the episodic overload of motor and cognitive circuits. Parieto-frontal networks are involved in visuo-driven locomotion and could be a key structure to explain this phenomenon. Previously we demonstrated that the frontal areas of this network were hypometabolic during gait in parkinsonian patients with freezing of gait, while parietal ones were hypermetabolic [2].
Objective
Our objective was to clarify the cerebral dysfunction of the frontal premotor regions in parkinsonian freezers.Methods
Resting-state MRI was performed in 10 freezer and 14 non-freezer patients matched for disease severity and cognitive status. Freezer patients were known to present hypometabolism of frontal areas during gait. Atrophy measures, anatomical connectivity (with ROIs in premotor and frontal eye field areas, and whole brain connectivity) and functional connectivity (from the same ROIs) were studied.Results
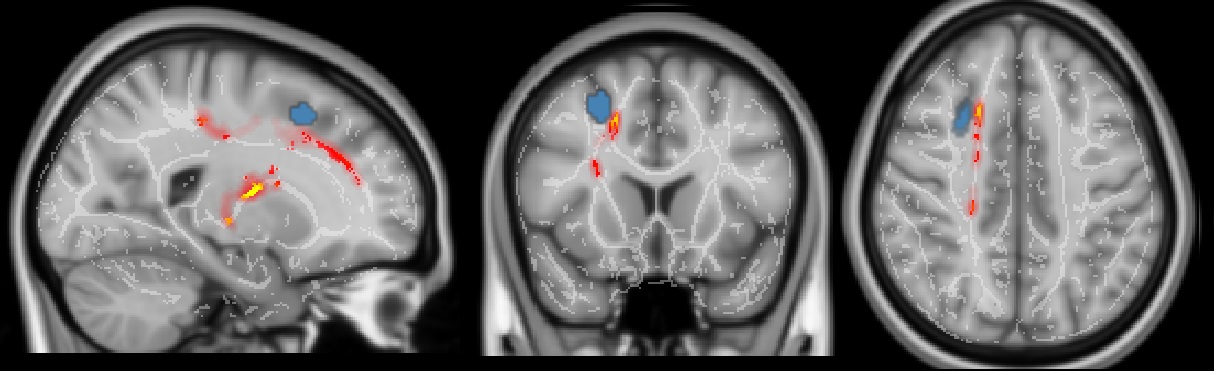
We found orbitofrontal atrophy in freezers patients. Concerning white matter, the premotor areas were anatomically disconnected from the cortical and subcortical structures, namely from the right FEF (only a tendency from left PMc). Then, functional MRI studies revealed a functional disconnection of the prefrontal cortex in FoG patients, at least from the left premotor cortex. Connectivity from the right FEF was preserved in the FoG group, contrasting with anatomic results.Conclusions
Multimodal imaging techniques helped us to better characterize the involvement of the prefrontal cortex in freezing. Atrophy was described in the orbitofrontal area, whereas white matter lesions were preponderant in the right prefrontal cortex and functional disconnection was major from the left one.
The destructuration of the right parieto-frontal network prevents the equilibrium between left and right networks. The anatomic disruption of the right parieto-frontal in freezers could enhance its dominance on the left parietofrontal network, via interhemispheric inhibitions. This imbalance between these two circuits could explain the preponderance of stimulus-driven attention on goal-driven attention in freezers [3].
Acknowledgements
No acknowledgement found.References
[1] Nutt JG, Bloem BR, Giladi N, Hallett M, Horak FB, Nieuwboer A. Freezing of gait: moving forward on a mysterious clinical phenomenon. Lancet Neurol. 2011 Aug;10(8):734-44.
[2] Tard C, Delval A, Devos D, Lopes R, Lenfant P, Dujardin K, Hossein-Foucher C, Semah F, Duhamel A, Defebvre L, Le Jeune F, Moreau C. Brain metabolic abnormalities during gait with freezing in Parkinson's disease. Neuroscience. 2015 Oct 29;307:281-301
[3] Corbetta M, Patel G, Shulman GL. The reorienting system of the human brain: from environment to theory of mind. . Neuron. 2008 May 8;58(3):306-24
Figures