1929
Brain morphological changes in early-stage Parkinson’s disease1Radiology, Penn State University College of Medicine, Hershey, PA, United States, 2Radiology, Shengjing Hospital of China Medical University, Shenyang, Liaoning, China, 3Neurology, Penn State University College of Medicine, Hershey, PA, United States, 4Neural & Behavioral Sciences, Penn State University College of Medicine, Hershey, PA, United States, 5Neurosurgery, Penn State University College of Medicine, Hershey, PA, United States
Synopsis
At disease onset clinically, the motor symptoms and signs are usually asymmetric or unilateral in majority of Parkinson’s disease (PD) patients. When disease progresses to a later stage, the asymmetry becomes less significant. The cause of this asymmetry, and the relationship between functional deficits and the structural changes in the brain are not clear. In this study, we investigated the morphological changes in the brain hemispheres corresponding to the early-onset and late-onset body sides through a longitudinal study on 24 early-stage PD patients. Significant atrophy was observed in the motor cortex and basal ganglia nuclei.
Background:
At disease onset clinically, the motor symptoms and signs are usually asymmetric or unilateral in majority of Parkinson’s disease (PD) patients, especially in early-onset patients with parkinsonian symptom onset younger than age 60. To this effect, postmortem pathological studies of early-stage PD have demonstrated the asymmetry in pathological status between the two hemispheres1. The tendency to develop a more symmetric system was associated with higher age and longer disease duration2,3. In addition, the data from previous morphological studies of PD were not consistent, with some reported significant atrophy in the cortex and basal ganglia nuclei4,5, while others reported no significant atrophy6. In this study, we investigated the morphological changes in the brain hemispheres corresponding to the early-onset and late-onset body sides through a longitudinal study on 24 early-stage PD patients.MATERIALS AND METHODS:
Human Subjects
Twenty-four right-handed H&Y stage I early-onset idiopathic PD subjects (age 55.7 ± 4.5 years, 8 females) were recruited and studied longitudinally for up to two years (1.9 ± 0.5 years). Ten subjects had their motor symptoms on their left body side (53.8 ± 5.3 years, 3 females); fourteen subjects on the right side (57.1 ± 3.3 years, 5 females). There was no significant difference in the age or sex distributions between the patients with different early-onset body sides. The motor function deficits were evaluated with the Part 3 of MDS-Unified Parkinson’s Disease Rating Scale (UPDRS-3). All subjects gave written informed consent, which was consistent with the Declaration of Helsinki, reviewed and approved by the Institutional Review Board of Penn State University College of Medicine.
Morphological MRI
Morphological MRI of the whole brain was conducted with a T1-weighted three-dimensional MPRAGE method on a Siemens Magnetom Trio 3 T system with an 8-channel head coil. The imaging parameters were TR/TE/FA = 2300 ms / 2.98 ms / 9°, FOV = 256 mm ´ 256 mm ´ 160 mm, acquisition matrix = 256 ´ 256 ´ 160, image resolution = 1 mm ´ 1 mm ´ 1 mm, and iPAT factor = 2. The morphological data were processed with a longitudinal pipeline and a longitudinal two stage model in FreeSurfer7. The longitudinal changes of the cortical thickness of motor cortex and the volume of basal ganglia structure (putamen, and caudate nucleus) were measured using FreeSurfer brain parcellation results. Interhemispheric comparison of cortical thickness and structural volume were conducted between left and right, and the hemispheres corresponding to the early and late-onset body side using paired t-test (p < 0.05).
RESULTS:
RESULTS:
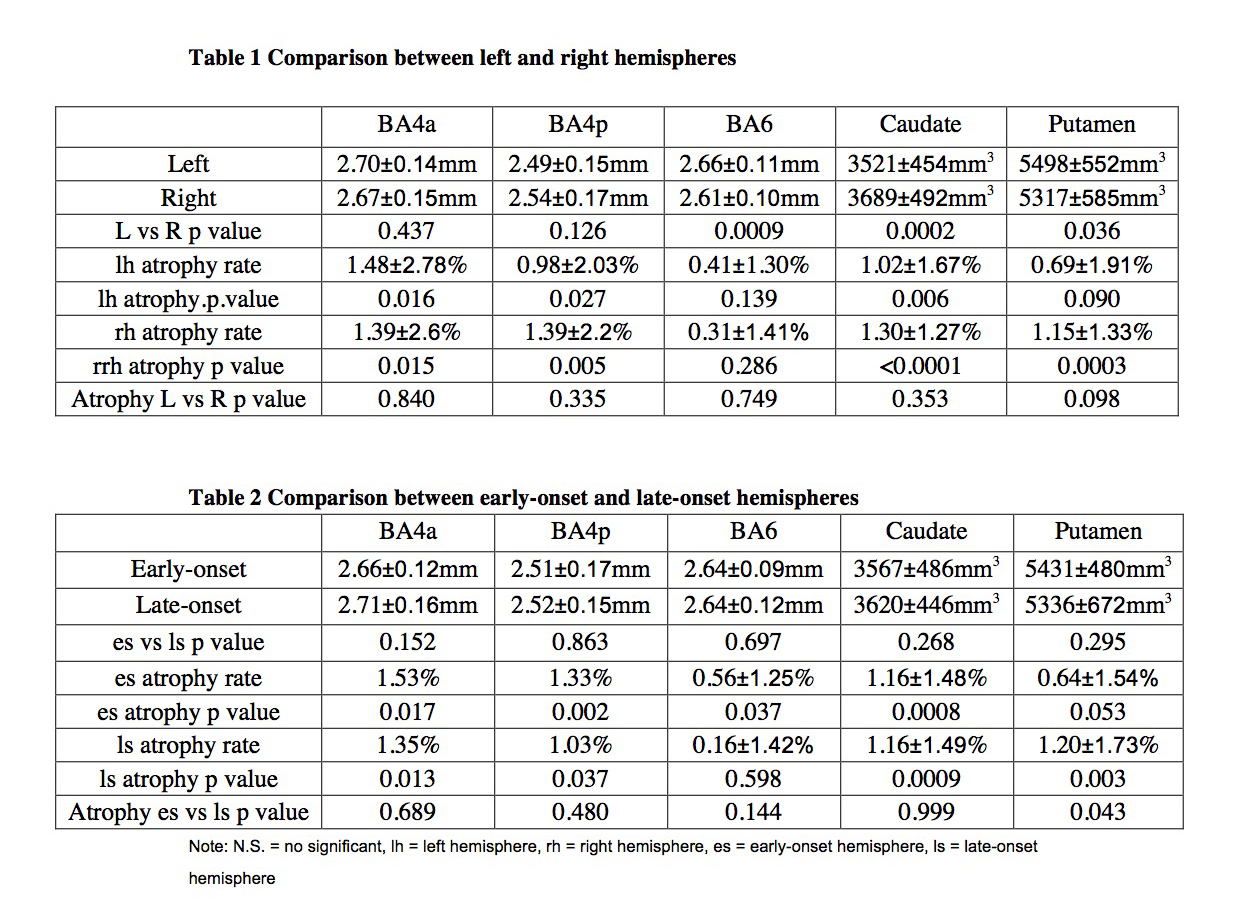
Left BA6 was thicker than the right hemisphere. Left putamen was
bigger than the right, and right caudate was bigger than the left (paired
t-test, p < 0.05). There was no significant difference between the early and
late-onset symptomatic hemispheres in cortical thickness or structural volume. In
two years after the first visit at stage I, BA4a, BA4p, caudate and putamen in
both left and right hemispheres, and also in the early and late-onset hemispheres,
showed significant atrophy (Table 1). Both left and right BA4, caudate, and
putamen showed significant atrophy, while there was no significant difference
between the atrophy rate in the two hemispheres. There was significant atrophy
in the early-onset and late-onset BA4 and caudate, early-onset BA6, and
late-onset putamen (Table 2). The atrophy rate in late-onset putamen is higher
than the early-onset side. Discussion & Conlusion:
The longitudinal changes in motor cortex thickness and subcortical
structure volume in PD may provide new
insights into the relation between clinical symptoms and the pathological
changes in the brain. During the disease progression in the early stages,
significant atrophy was observed in the motor cortex and basal ganglia nuclei. Even
though we did not expect significant aging-related brain atrophy within two
years, aging effect cannot be excluded. The human brain mean atrophy rate is
0.45% per year (from 20 years to 80 years) and is 0.31% at 60 years8,
which is less than our result. The PD patients whole brain atrophy is 0.71% per
years, and putamen atrophy is 1.2% – 2.1% per year9,10. The Further
study is needed to include an age-match healthy control group. These results
demonstrate the sensitivity to use morphological MRI to monitor the disease
progression in the early stage of PD. Acknowledgements
This study was supported by the DANA Foundation, and the Department of Radiology, Pennsylvania State University College of Medicine.References
1. Kempster PA, Gibb WR, Stern GM, Lees AJ. Asymmetry of substantia nigra neuronal loss in Parkinson's disease and its relevance to the mechanism of levodopa related motor fluctuations. J Neurol Neurosurg Psychiatry. 1989 Jan;52(1):72-6.
2. Marinus J, van Hilten JJ. The significance of motor (a)symmetry in Parkinson's disease. Mov Disord. 2015 Mar;30(3):379-85.
3. Go´mez-Esteban JC, Tijero B, Ciordia R, et al. Factors influencing the symmetry of Parkinson’s disease symptoms. Clin Neurol Neurosurg 2010; 112:302–05 CrossRef Medline
4. Nemmi F, Sabatini U, Rascol O, Péran P. Parkinson's disease and local atrophy in subcortical nuclei: insight from shape analysis. Neurobiol Aging. 2015 Jan; 36(1):424-33.
5. Geng DY, Li YX, Zee CS. Magnetic resonance imaging-based volumetric analysis of basal ganglia nuclei and substantia nigra in patients with Parkinson's disease. Neurosurgery. 2006 Feb;58(2):256-62; discussion 256-62.
6. Hwang I, Sohn CH, Kang KM, Jeon BS, Kim HJ, Choi SH, Yun TJ, Kim JH. Differentiation of Parkinsonism-Predominant Multiple System Atrophy from Idiopathic Parkinson Disease Using 3T Susceptibility-Weighted MR Imaging, Focusing on Putaminal Change and Lesion Asymmetry. AJNR Am J Neuroradiol. 2015 Dec;36(12):2227-34.
7. M. Reuter, N.J. Schmansky, H.D. Rosas, B. Fischl. Within-Subject Template Estimation for Unbiased Longitudinal Image Analysis. NeuroImage 61(4), pp. 1402-1418, 2012.
8. Lockhart SN, DeCarli C. Structural imaging measures of brain aging. Neuropsychol Rev. 2014 Sep;24(3):271-89.
9. Melzer TR, Myall DJ, MacAskill MR, Pitcher TL, Livingston L, Watts R, Keenan RJ, Dalrymple-Alford JC, Anderson TJ. Tracking Parkinson's Disease over One Year with Multimodal Magnetic Resonance Imaging in a Group of Older Patients with Moderate Disease. PLoS One. 2015 Dec 29;10(12):e0143923.
10. Elijah Mak, Li Su, Guy B. Williams, Michael J. Firbank, Rachael A. Lawson, Alison J. Yarnall, Gordon W. Duncan, Adrian M. Owen, Tien K. Khoo, David J. Brooks, James B. Rowe, Roger A. Barker, David J. Burn, John T. O’Brien. Baseline and longitudinal grey matter changes in newly diagnosed Parkinson’s disease: ICICLE-PD study. Brain. 2015 Oct; 138(10): 2974–2986.
Figures