1922
Decreased Cerebral Blood Volume among those with Chronic Brain Insult in HIV1Huntington Medical Research Institutes, Pasadena, CA, United States, 2Phil Simon Clinic, Pasadena, CA, United States
Synopsis
Despite advances in medications and modern practices of immediate antiretroviral therapy, chronic HIV infection remains associated with brain insults, cognitive decline, and related neurological disorders. Reduced N-acetyl-aspartete (NAA), a metabolic marker of neuronal injury, was associated with advanced age and lower CD4 nadir count in a chronic, asymptomatic HIV cohort. Using a novel, BOLD MR protocol incorporating hypercapnic and hyperoxic stimuli, NAA showed no relation to cerebrovascular reactivity (CVR) but was significantly correlated to cerebral blood volume (CBV). Our results may indicate future use of NAA and CBV as complementary non-invasive metrics to track brain health in HIV.
Introduction
In this modern era, HIV can be effectively suppressed with antiretroviral therapy without developing Acquired Immunodeficiency Syndrome. However, chronic HIV infection is often associated with brain insults, cognitive decline and HIV-associated neurological disorders. Two important brain hemodynamic measures impacted in virally suppressed HIV, particularly in the presence of associated neurological disorders, are cerebrovascular reactivity (CVR), a measure of endothelial function, and cerebral blood volume (CBV), related to vascular density and vasodilation.2 The relation of these measures to chronic brain health in well-controlled HIV is uncertain. Here we use a novel, advanced gas-inhalation MR protocol to evaluate the independent associations of CVR and CBV changes with evidence of brain insult in chronic HIV.1 Brain insult in HIV has been quantified by decline in the MR Spectroscopy metabolic marker N-acetyl-aspartate (NAA) which reflects neuronal integrity.5 We first verify NAA is a reliable surrogate marker of brain insult in an era of more effective and aggressive antiretroviral therapy, by studying the association with advanced age and lower CD4 nadir which are linked with increased brain insult in chronic HIV infection. We then tested the hypothesis that reduced NAA would be correlated with brain hemodynamic dysfunction, quantified by reduced CVR and CBV.Methods
We studied twenty-six HIV-positive patients (ages 25-77), two with AIDS risk (CD4 count < 200) but none have known central nervous system (CNS) manifestations. Simultaneous response to hypercapnic and hyperoxic stimulus on BOLD fMRI with a GE 3T scanner through administration of room air, 5% CO2, 95% O2, and a mixture of the latter gases in a varied block-timing schedule to identify endothelial-dependent increase in blood flow and oxygen-saturation effects to reduce deoxyhemoglobin. A general linear model is generated in FMRIB Software Library (FSL 5.0.7) to regress end tidal data with the BOLD timeseries to produce parameter estimates for CVR and CBV. We acquired MR spectroscopy data using short echo time point-resolved spectroscopy (PRESS) technique in five brain regions: posterior gray matter, frontal GM, parietal white matter, frontal WM, and basal ganglia3,4 for analysis using Linear Combination of Model (LCM, 2016); NAA/Cr+PCr was standardized into z-scores and averaged over the five brain regions. Statistical analysis was performed on JMP Pro in which NAA was fit with age and CD4 nadir to confirm its reliability as a marker of brain insult, and with CVR and CBV to identify association with hemodynamic dysfunction.Results
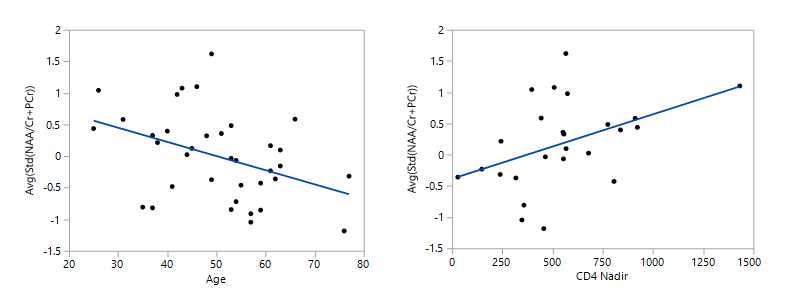
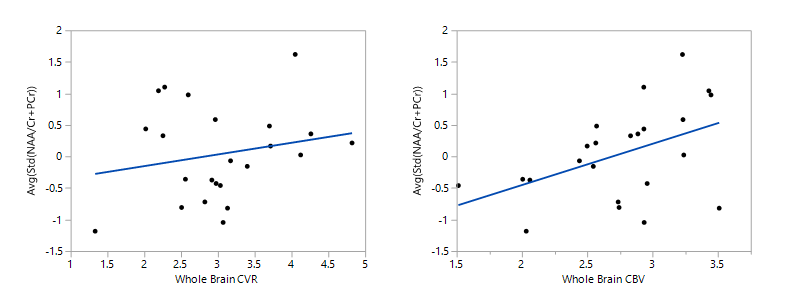
NAA levels decreased with lower CD4 nadir (0.0010±0.0004, p=.03) and advanced age (-0.022±0.009, p=.01). CVR was not significantly associated with NAA (p=.3) but decreased CBV was significantly associated with lower NAA (0.52±0.23, p=.03).Discussion
Our findings confirmed a reduction in NAA as a surrogate measure of brain insult in our chronic HIV-infected cohort by correlation to established clinical predictors of advanced age and lower CD4 nadir. This is important as the field of HIV treatment has rapidly evolved; earlier initiation of treatment results in fewer individuals developing AIDS. Having confirmed variance in brain integrity, we then evaluated their associations with sensitive measures of brain hemodynamic function. We did not find a significant relation between NAA and CVR, indicating that endothelial dysfunction is not a prominent feature of brain insult in chronic-HIV. However, we did see a decline in CBV related to reduction in NAA. HIV is well known to cause vascular damage in the systemic and cerebral circulation. Never entirely cleared from the brain, persistent subclinical alterations of the immune system by chronic HIV infection may damage blood vessels even after systemic viral suppression. A reduction in CBV may also reflect decreased perfusion secondary to decline in brain function. More research must be performed with additional vascular parameters to distinguish these associations and establish whether blood vessel alterations contribute prospectively to decline in NAA and other measures of subclinical brain insult.Conclusion
Our work affirms the significant correlation of brain hemodynamic dysfunction in HIV with measures of brain insult. In chronic HIV, NAA and CBV can be used as functional, non-invasive metrics to trace variance in brain impact. If CBV reduction is established as an important contributor to brain insult, this may point the way towards new vascular approaches to promote brain health and to monitor efficacy in chronic HIV.Acknowledgements
No acknowledgement found.References
1. Liu, P., et al., 2016. "Multiparametric imaging of brain hemodynamics and function using gas-inhalation MRI. " NeuroImage, 146: 715-723.
2. Chow, F.C., et al., 2016. "Cerebral vasoreactivity is impaired in treated, virally suppressed HIV-infected individuals. " AIDS, 30(1): 45-55.
3. Mohamed, M.A., et al., 2010. "Brain metabolism and cognitive impairment in HIV infection: a 3 Tesla Magnetic Resonance Spectroscopy Study. " Magn Reson Imaging, 28(9): 1251-1257.
4. Paul, R.H., et al., 2007. "Proton MRS and Neuropsychological Correlates in AIDS Dementia Complex: Evidence of Subcortical Specificity." J Neuropsychiatry Clin Neurosci, 19(3): 283-292.
5. Paul, R. H., et al., 2008. "Relative sensitivity of magnetic resonance spectroscopy and quantitative magnetic resonance imaging to cognitive function among nondemented individuals infected with HIV." J Int Neuropsychol Soc 14(5): 725-733.
Figures