1920
Territory Arterial Spin Labeling technique in evaluation of Superficial Temporal Artery to Middle Cerebral Artery Bypass Surgery in Moyamoya Disease1RADIOLOGY, BEIJING TIANTAN HOSPITAL,CAPITAL MEDICAL UNIVERSITY, BEIJING, China, 2MR RESEARCH CHINA, GE HEALTHCARE, BEIJING, China
Synopsis
The purpose of this study was to evaluate cerebral blood flow and territory through superficial temporal artery (STA) to middle cerebral artery (MCA) bypass in patients with Moyamoya disease after direct revascularization surgery using territory arterial spin labeling (tASL) technique. ASL and tASL scan were performed before and after bypassing surgery. our study demonstrated some bypasses can effectively supply blood flow into the brain and others cannot. tASL technique can selectively demonstrate perfusion territory through STA to MCA bypass. Thus, provide information about patency of STA to MCA bypass.
INTRODUCTION
Bypassing surgery is a conventional treatment method for Moyamoya disease (MMD). Superficial temporal artery (STA) and middle cerebral artery (MCA) are connected to release the cerebral perfusion burden. Efficiency evaluation of the newly established branch is of critical clinical value. Both intraoperative fluorescein angiography and postoperative CT or MR angiography (CTA, MRA) have been used to observe whether STA and MCA were successfully connected or not. Traditional perfusion imaging, like arterial spin labeling (ASL)1-2, and dynamics susceptibility contrast (DSC) was also used to assess the hemodynamic improvement. Yet, with these techniques, it remains impossible to evaluate the amount of blood flow introduced into the MCA branch and the corresponding fed region. Saida et al3 has used multiphase selective ASL technique in evaluation of revascularization surgery in a very limited number of MMD patients. In this work, we used territorial ASL (tASL) and standard pseudo continuous ASL to evaluate the hemodynamic change and affected region after revascularization.
METHODS
Twenty-three diagnosed MMD patients were treated by unilateral STA to MCA bypass surgery and included in this study. ASL and tASL examinations were performed before surgery and during early postoperative period (within 7 days). Both ASL and tASL were acquired with 3D stack of spiral fast spin echo sequence. The parameters for ASL and tASL were as follows, labeling duration 1450ms, post labeling delay 2025ms. CBF was measured from ASL perfusion map. Bilateral internal carotid artery (ICA), bilateral external carotid artery (ECA) and vertebrobasilar artery (VBA) were labelled via super-selective scheme. Postoperative unilateral ECA perfusion weighted images were used to check if there was blood flow from bypass to MCA territory. According to whether there was blood flow from bypass, the patients were divided into positive and negative groups. In positive group, pre- and postoperative CBF was measured in bypass supplied area. In negative group, pre- and postoperative CBF was measured in MCA territory. The Wilcoxon signed-rank test was used to evaluate the difference in pre- and postoperative CBF in positive and negative groups respectively.RESULTS
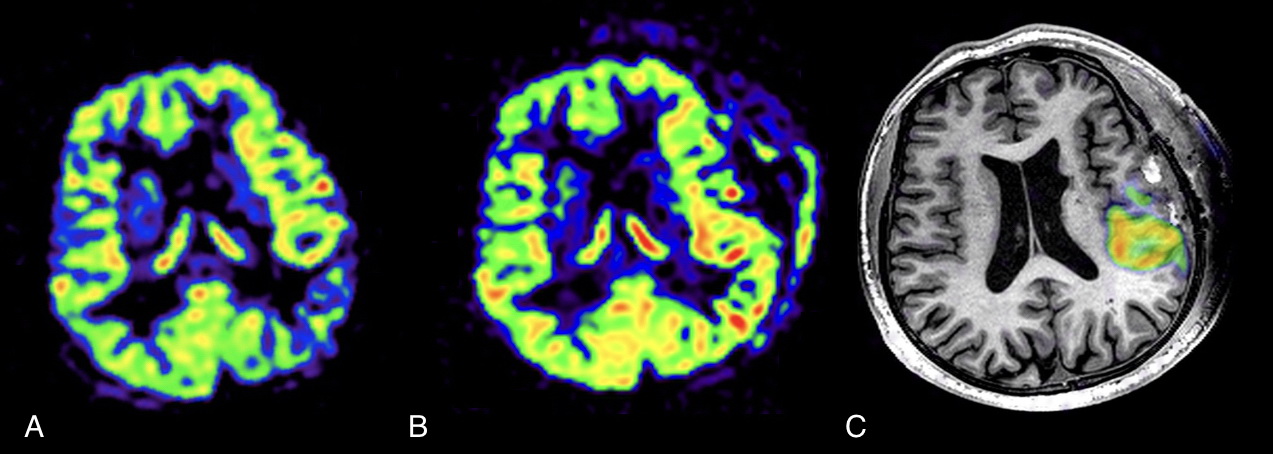
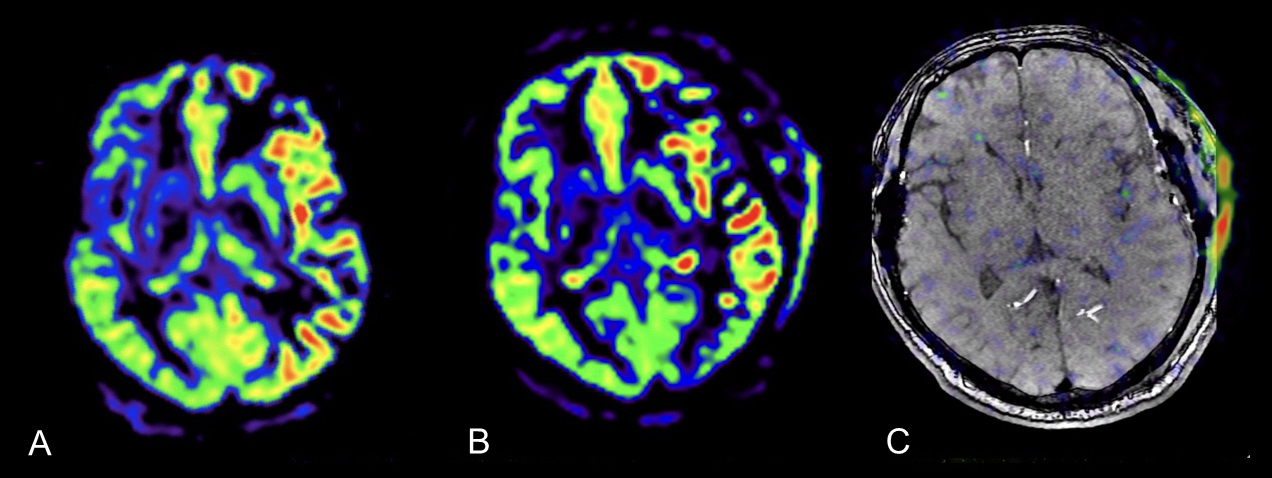
In thirteen of 23 patients, early postoperative tASL examinations demonstrated blood flow through bypass to MCA distribution. Postoperative CBF measured by ASL were significant higher than before (P=0.01,<0.05). In the remaining 10 patients, early postoperative tASL examinations failed to demonstrate blood flow through bypass into brain. Postoperative CBF showed no statistical significant than before (P=0.48, >0.05).DISCUSSION
All the patients included in our study have been proved that bypasses were patent by fluorescein angiography. Postoperative CTA (not shown in this study) also showed the connection of STA and MCA branches in these patients. Yet, tASL results suggested that among these patent bypasses, some bypasses can effectively supply blood flow into the brain and others cannot. So, we speculated that in early postoperative period, some bypasses are not ‘functional’, that is, no or less supply blood from STA to MCA, even if they are proved patent by other imaging techniques. tASL gives selective perfusion map of bypass in a noninvasive manner. Unlike other methods which evaluate morphology and patency of bypass, we suggest tASL evaluate efficacy of bypass. Not all patent bypass show efficacy in early postoperative period. On the other hand, in those patients whose bypass give blood supply into the brain, bypass is surely patent. The limitation of our study was that we lack long term postoperative follow up of these MMD patients. For those bypasses which didn’t give blood supply into brain parenchyma in early postoperative period, contemporarily we do not know whether those bypasses can give blood supply in long term postoperative period.CONCLUSION
tASL technique can selectively demonstrate perfusion territory through STA to MCA bypass. This information can prove that STA to MCA bypass is patent and supply blood to brain parenchyma. As a non-invasive, non-radiation examination and no contrast medium is needed, tASL is a useful technique in evaluation of direct revascularization surgery in MMD.Acknowledgements
No acknowledgement found.References
1.Blauwblomme T, Lemaitre H, Naggara O, et al. Cerebral Blood Flow Improvement after Indirect Revascularization for Pediatric Moyamoya Disease: A Statistical Analysis of Arterial Spin-Labeling MRI. AJNR Am J Neuroradiol. 2016; 37(4): 706-12.
2.Hara S, Tanaka Y, Ueda Y, et al. Noninvasive Evaluation of CBF and Perfusion Delay of Moyamoya Disease Using Arterial Spin-Labeling MRI with Multiple Postlabeling Delays: Comparison with (15)O-Gas PET and DSC-MRI. AJNR Am J Neuroradiol. 2017; 38(4): 696-702.
3.Saida T, Masumoto T, Nakai Y, et al. Moyamoya disease: evaluation of postoperative revascularization using multiphase selective arterial spin labeling MRI. J Comput Assist Tomogr. 2012; 36(1): 143-9.
Figures