1910
Imaging Patterns and Implications of Time-of-Flight Magnetic Resonance Angiography in Intracranial Atherosclerotic Stenosis1Department of Radiology, Chinese PLA General Hospital, Beijing, China, 2Department of Interventional Radiology, Beijing Tiantan Hospital, Beijing, China
Synopsis
The imaging pattern and implication of intracranial atherosclerotic stenosis on TOF MRA had not been fully understood. In patients with middle cerebral artery stenosis, we had used high-resolution vessel wall imaging to evaluate plaque morphology and conventional angiography to evaluate cerebral hemodynamics in groups with different TOF MRA pattern. We had found that the TOF MRA pattern was associated with stenosis percentage, the middle cerebral artery branch signal intensity distal to the site of stenosis on TOF MRA was associated with hemodynamic impairments and was determined by the status of antegrade flow.
INTRODUCTION
Three-dimensional time-of-flight (TOF) Magnetic resonance angiography (MRA) had been widely applied to evaluate the severity of symptomatic or asymptomatic intracranial atherosclerotic stenosis (ICAS). However, the implication and underlying mechanism of different imaging patterns were not well studied. In the present study, we aimed to assess the vessel wall abnormalities and cerebral hemodynamics in the different pattern of middle cerebral artery moderate to severe stenosis and thus to explore the implication of imaging patterns revealed by TOF MRA.METHODS
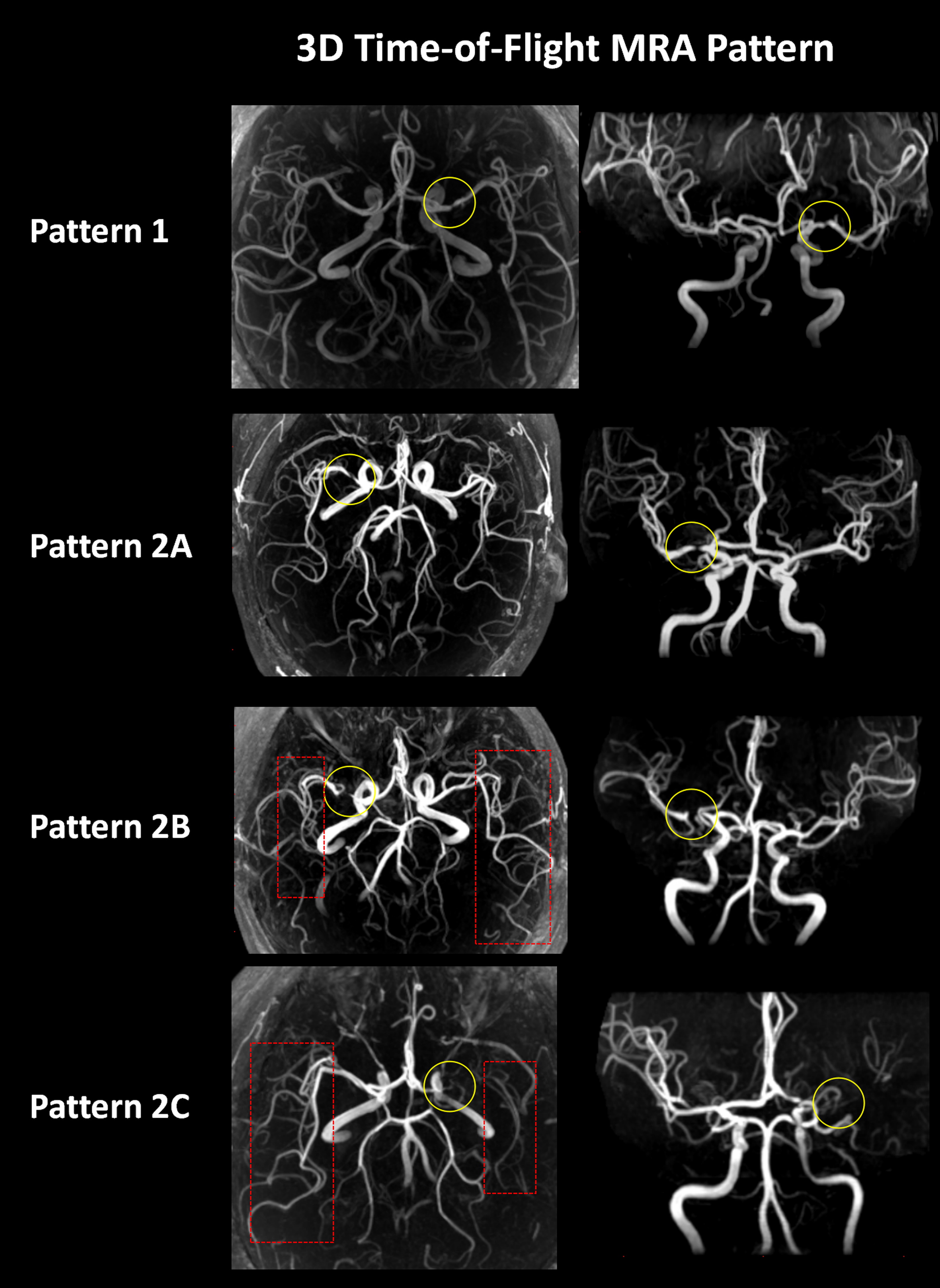
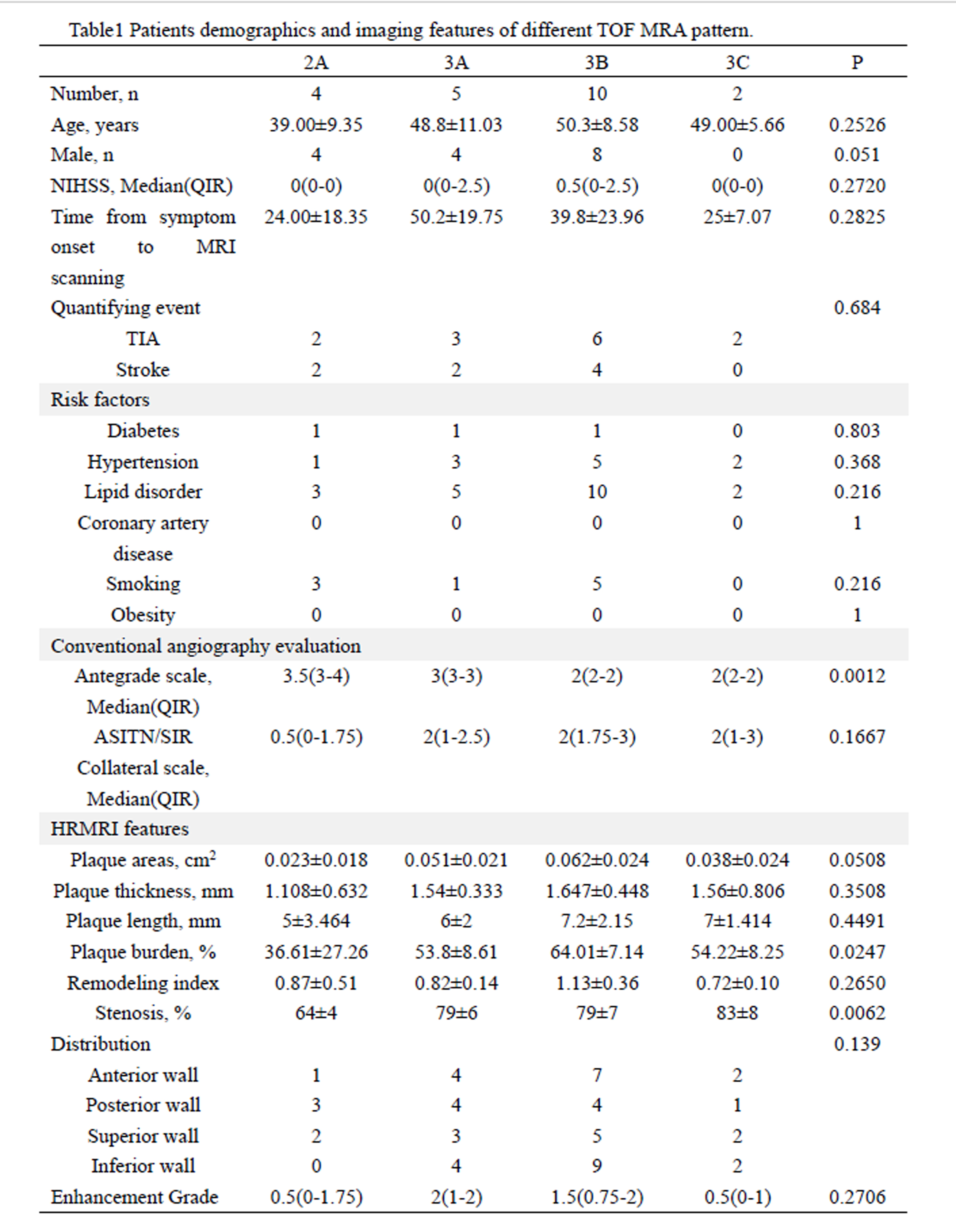
Patients with unilateral middle cerebral artery (MCA) atherosclerotic moderate to severe stenosis confirmed by conventional angiography were enrolled in this study from August 2013 to November 2014. Patients with multiple MCA and/or extracranial internal carotid artery stenosis/occlusion were excluded. Patients' clinical demographics and risk factors were recorded. All patients had underwent vessel wall high-resolution MRI (HRMRI) and 3D TOF MRA. Imaging patterns revealed by TOF MRA were classified as 2 grades: mild to moderate (grade 1, focal signal reduction >50% and lumen stenosis) and severe (grade 2, signal loss with the distal flow). The MCA branch signal intensity distal to the site of stenosis on TOF MRA was classified as either good (grade A) or poor [mild reduction (grade B) or severe reduction (grade C)] according to the extent to which the MCA could be visualized.1 Figure 1 represent typical cases of the imaging patterns. HRMRI was used to quantify the morphological parameters of target lesion including plaque length, thickness, plaque area, plaque burden, stenosis percentage and arterial remodeling index at maximal lumen narrowing site.2 Conventional angiography was used to evaluate antegrade flow and collateral flow according to modified TICI scale and ASITN/SIR collateral scale.3 Clinical demographics, risk factors, HRMRI and hemodynamic parameters were compared between the different TOF MRA patterns.RESULTS
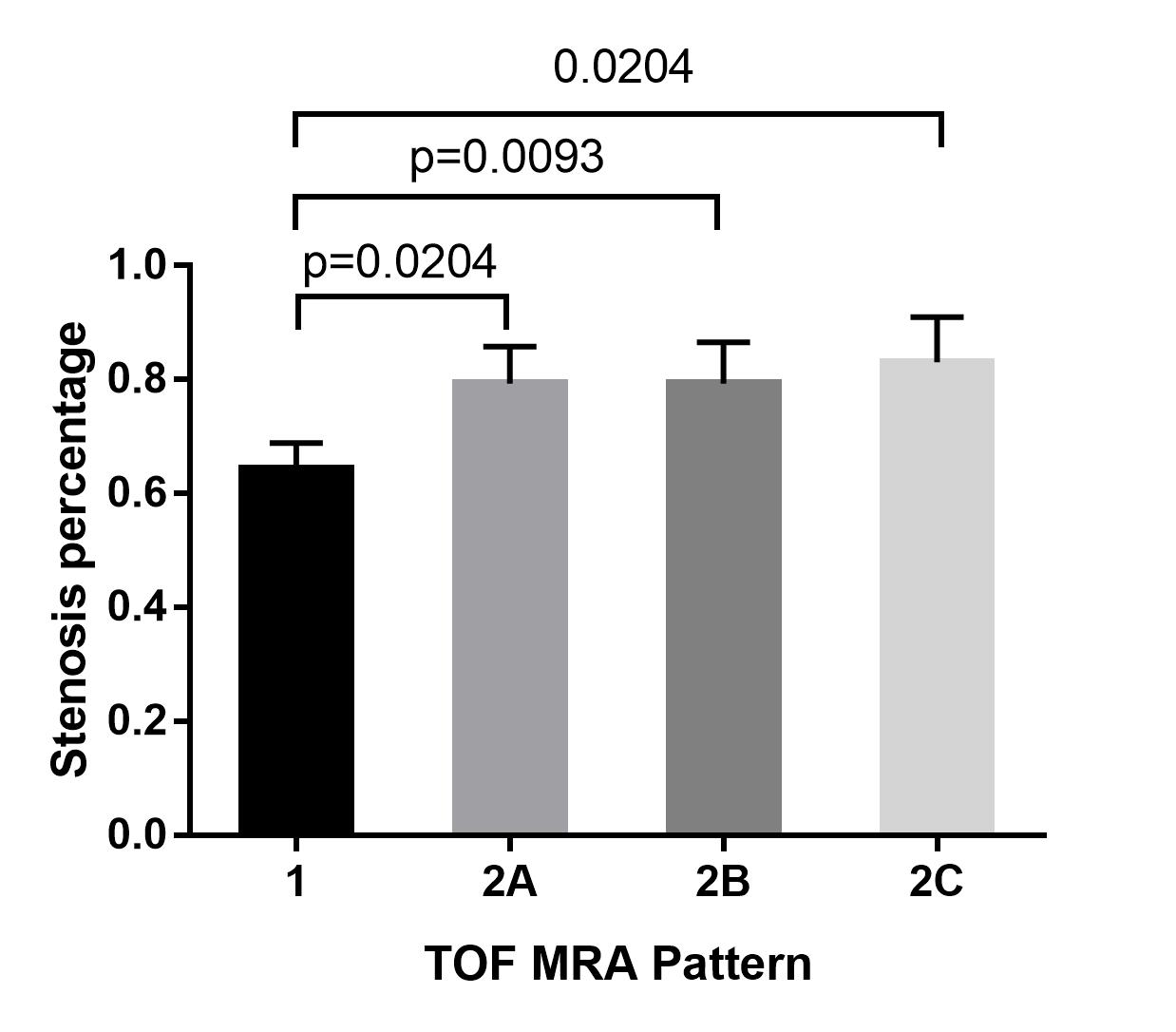
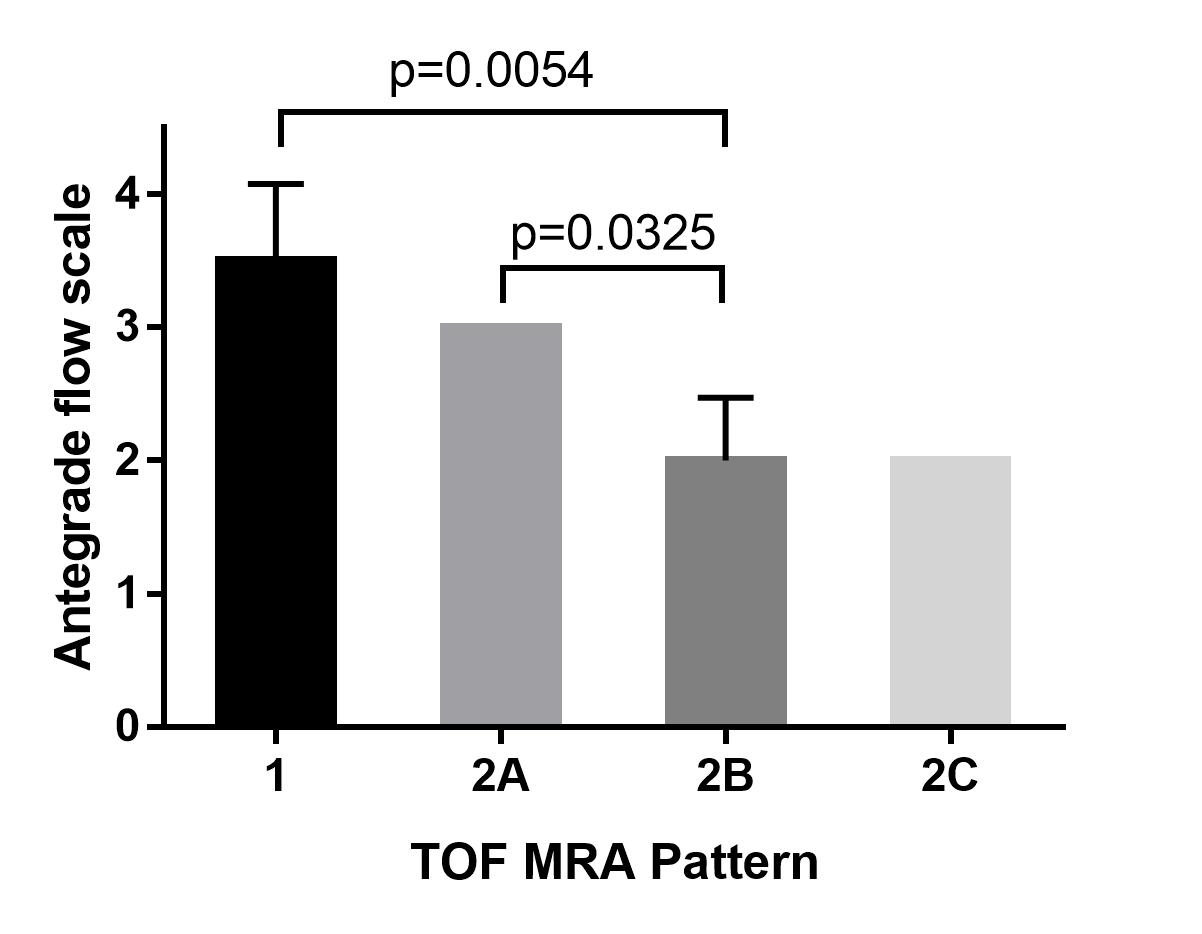
Twenty-one patients (47.67±9.55 years, 5 females) were included in this study. Four patients were assessed as grade 1 and 17 patients were assessed as grade 2. In grade 2, 5 patients were assessed as 2A, 10 patients were assessed as 2B and 2 patients were assessed as 2C. Patients were categorized as group 1, group2A, group 2B and group 2C. For HRMRI, stenosis percentage was significantly different between groups (Figure 2 represents results of multiple comparisons). For hemodynamic evaluation, antegrade flow scale was significantly different between groups (Figure 3 represents results of multiple comparisons). Collateral circulation was not significantly different between the groups. Additionally, clinical demographics and risk factors were not significantly different. Details please see Table 1.CONCLUSION
TOF MRA qualifies with morphology features of stenosis lesion and is useful to assess the severity of ICAS. The MCA branch signal intensity distal to the site of stenosis on TOF MRA is associated with hemodynamic impairments and is determined by the status of antegrade flow. More robust antegrade flow is related to a better appearance of the distal branches on TOF MRA, which may be used as a feasible imaging marker to assess reperfusion/recanalization in acute stroke.Acknowledgements
NoneReferences
1.Chen H, Li Z, Hong H, et al. Relationship between visible branch arteries distal to the stenosis on magnetic resonance angiography and stroke recurrence in patients with severe middle cerebral artery trunk stenosis: a one-year follow up study[J]. BMC Neurology, 2015, 15(1): 167-167.
2.Ma N, Jiang W J, Lou X, et al. Arterial remodeling of advanced basilar atherosclerosis A 3-tesla MRI study[J]. Neurology, 2010, 75(3): 253-258.
3.Zaidat O O, Yoo A J, Khatri P, et al. Recommendations on Angiographic Revascularization Grading Standards for Acute Ischemic Stroke A Consensus Statement[J]. Stroke, 2013, 44(9): 2650-2663.
Figures