1908
7T TOF-MRA showed a decreased contrast-to-noise ratio of the lenticulostriate arteries in hemispheres with unilateral lacunar stroke1State Key Laboratory of Brain and Cognitive Science, Institute of Biophysics, Chinese Academy of Sciences, Beijing, China, 2University of Chinese Academy of Sciences, Beijing, China, 3The Innovation Center of Excellence on Brain Science, Chinese Academy of Sciences, Beijing, China, 4Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, China, 5Siemens Shenzhen Magnetic Resonance Ltd., Shenzhen, China
Synopsis
7T TOF-MRA has demonstrated an exquisite capacity for imaging the lenticulostriate artery (LSA) due to its high spatial resolution and in-flow effect. However, due to the morphological variability of the LSA, a clinical application is needed to identify abnormalities of this vessel. In this study, we analyzed the LSA using 7T TOF-MRA on patients with unilateral lacunar stroke. Comparing the results with other morphological parameters, we found that a reduced contrast-to-noise ratio (CNR) was a more sensitive parameter for reflecting impairment of the LSA on the ipsilateral side of the lacunae.
Introduction
The lenticulostriate artery (LSA) supplies the basal ganglia (BG) and its vicinity. Impairment of the LSA is a major cause of lacunar stroke in the BG and lateral ventricles (LV)1. Noninvasive imaging of the LSA is clinically useful to understand the mechanisms of microvascular pathologies and guide early therapeutic intervention. 7T TOF-MRA has shown an exquisite capacity for imaging the lenticulostriate artery due to its high spatial resolution and in-flow effect2. In this study, we imaged the LSA using high-resolution 7T TOF-MRA in patients with unilateral lacunar stroke and quantitatively analyzed the LSA on the ipsilateral and contralateral sides of the lacunae.Method
Four patients with unilateral infarcts in the BG and LV regions were enrolled in this study, with a confirmed clinical diagnosis collected prospectively. The local IRB approved the study, and informed consent was obtained from all the participants. All the images were acquired on a 7T research system (Siemens Healthcare, Erlangen, Germany) equipped with a Nova 32-channel head coil. The subjects underwent TOF-MRA, diffusion-weighted imaging (DWI), T1w, and FLAIR imaging.
The TOF-MRA was positioned to cover the middle cerebral artery (MCA) and LSA. The following parameters were used: FA = 20°, TR = 15 ms, TE = 4.30 ms, voxel = 0.23x0.23x0.36 mm3, FOV = 180x135x47 mm3, GRAPPA = 2, and TA = 7:34 min.
The DWI, T1w, and FLAIR images were inspected in OsiriX to identify the lacunar infarction. Vascular tracing of the MCA and LSA originating from M1 segments was manually conducted in SimVascular. The length and distance between the root and the extremity of the vascular branch were measured, and the tortuosity was calculated as the ratio of length to distance. Three branches with longest lengths in every hemisphere were selected to measure the contrast-to-noise ratio (CNR). The CNR was calculated at the sections of the LSA with vertical distances of 5, 10, and 15 mm from the MCA. The CNR was defined as [ max(SignalLSA) - mean(Signaltissue) ] / stdNoise.
Results
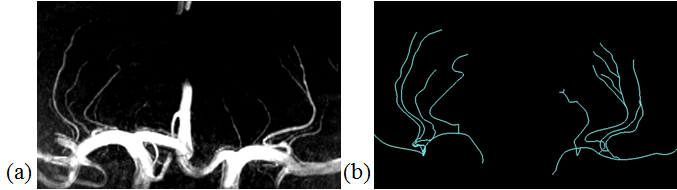
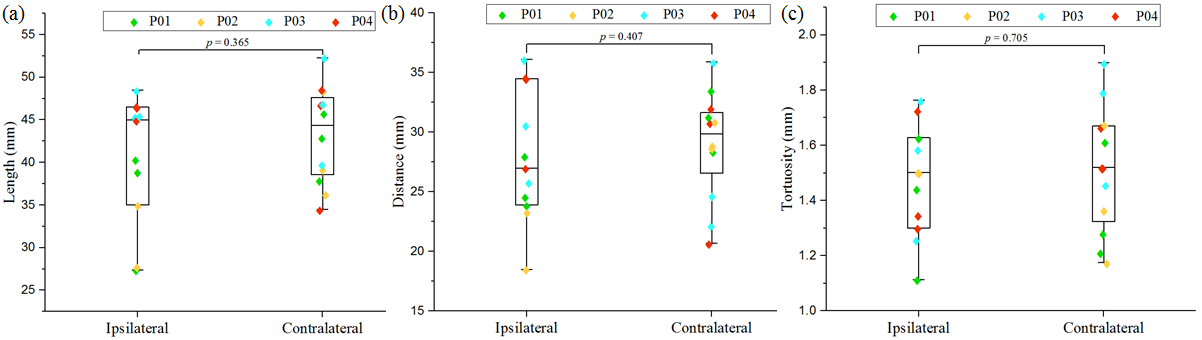
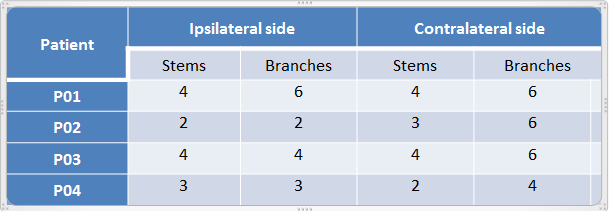
The extracted vascular trees were visually in good agreement with the coronal maximal intensity projection (MIP) of the TOF-MRA (Fig. 1). The numbers of stems and branches of the LSA are listed in Table 1. Independent sample t-tests showed no significant difference in the number of stems (p=1.000) or the number of branches (p=0.374) between the ipsilateral side (IPS) and the contralateral side (CON) of the lacunar infarction. There was also no significant difference between the IPS and CON sides in the length (p=0.365), distance (p=0.407), or tortuosity (p=0.705) of the three longest branches, as displayed in the box-scatter plots in Fig 2.
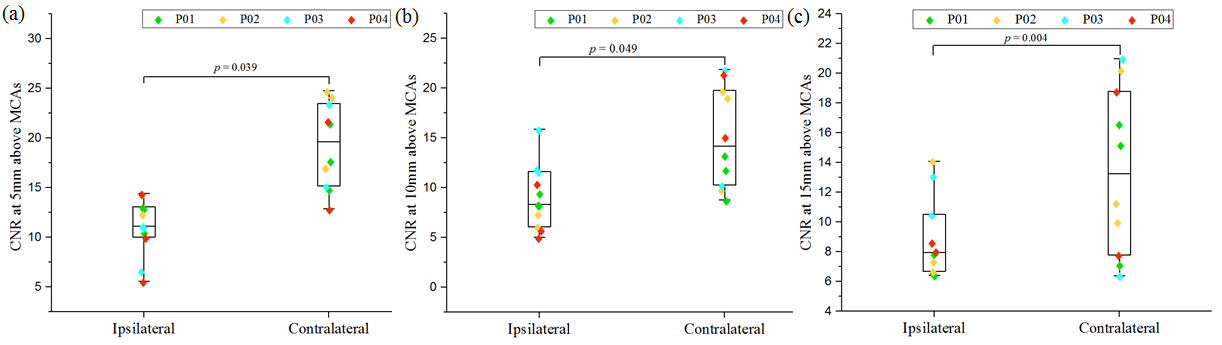
The box-scatter plot of the CNR was shown in Fig. 3, and it demonstrated
a significantly lower CNR on the IPS side than on the CON side at all locations
of measurement (p= 0.039 at 5 mm, p= 0.049 at 10 mm, and p= 0.004 at 15 mm). The CNR of the LSA branches decreased with increasing
distance from the parent MCA, on both the IPS and CON sides.
Discussion
As an angiographic imaging technique, the contrast of TOF-MRA derives from the in-flow effect of blood flow. Therefore, the impairment of vessels will initially affect the signal intensity in TOF-MRA. Our results showed that the CNR on the IPS side was significantly lower than that on the CON side, indicating that the lacuna was caused by the lesions in the ipsilateral LSA. Meanwhile, other quantitative parameters failed to reveal the difference in the LSA between IPS and CON sides.
Since 7T TOF-MRA was initially developed for imaging the LSA, many
parameters have been defined to quantify the LSA, including the number of stems
and branches, as well as its length, distance, and tortuosity. However, these
parameters can barely reveal the difference between an impaired LSA and a normal
one because of the great morphological differences of the LSA among
individuals. Previous research has suggested that the number of branches was
slightly lower in patients with chronic stroke compared with healthy
volunteers, and this conclusion was made after studying a relatively large sample
(n=10)3. Our study demonstrates that the CNR is a sensitive parameter
reflecting lesion of LSA in patients with unilateral lacunar stroke. The CNR could therefore be used as an indicator to evaluate the blood
supply of the LSA. Further studies using a larger sample size are needed to
evaluate the CNR of the LSA in healthy controls.
Conclusion
We demonstrated that the CNR of the LSA on the ipsilateral side of a lacunar stroke was lower than that on the contralateral side. The CNR is therefore a sensitive parameter to evaluate the blood supply of the LSA in high resolution TOF-MRA at 7T.Acknowledgements
This work was supported in part by the Ministry of Science and Technology of China grant(2015CB351701), and the National Nature Science Foundation of China grant (91132302)References
1. Gold G, Kovari E, Hof PR, Bouras C, Giannakopoulos P. Sorting out the clinical consequences of ischemic lesions in brain aging: a clinicopathological approach. J Neurol Sci 2007; 257:17–22.
2. Cho ZH, Kang CK, Han JY et al. Observation of the lenticulostriate arteries in the human brain in-vivo using 7.0T MR Angiography. Stroke 2008; 39:1604–6.
3. C-K Kang, C-A Park, C-W Park, Y-B Lee, Z-H Cho, Y-B Kim Lenticulostriate arteries in chronic stroke patients visualised by 7 T magnetic resonance angiography. Int J Stroke 2010; 5:374-380.
Figures