1873
Simultaneous acquisition of T1- and T2-weighted images using Volumetric Isotropic Turbo spin echo Acquisition (VISTA): A feasibility study towards cerebral venous thrombus imagingYunduo Li1, Shuo Chen1, Zechen Zhou2, Rui Li1, and Chun Yuan1,3
1Center for Biomedical Imaging Research, Department of Biomedical Engineering, Tsinghua University, Beijing, China, 2Philips Research North America, Cambridge, MA, United States, 3Department of Radiology, University of Washington, Seattle, WA, United States
Synopsis
This study demonstrated the feasibility of simultaneously acquiring T1 and T2-weighted images using dual-echo VISTA sequence. Phantom experiments showed that dual-echo VISTA can provide T1- and T2-weighted images as conventional T1/2 imaging sequences, and the performance of proposed sequence was further validated by in-vivo scan. By assembling flow-suppression, T1 and T2 contrast in one sequence, dual-echo VISTA has its potential to differentiate stages of thrombus more accurately.
Introduction
Cerebral venous thrombosis (CVT) is a relatively uncommon form of stroke that usually afflicts younger patients1. Conventional imaging diagnosis of venous thrombus requires a combination of various imaging modalities, such as computed tomography (CT), magnetic resonance (MR), MR venography (MRV), and conventional x-ray angiography, resulting a diagnostic delay in patients2. Previous studies showed that MR ‘black-blood’ imaging, as a noncontrast-enhanced T1-weighted imaging technique, can achieve detection of cerebral venous thrombus3. However, T1-weighted ‘black-blood’ MR imaging has difficulties when differentiating stages of thrombus, such as hyperacute (< 24 hours) and chronic (> 14 days) thrombosis, both of which exhibit isointense signal in T1-weighted images. Thus, multi-contrast MR imaging techniques are needed for more accurate identification of thrombus. In this study, we combined T1- and T2- contrast in Volumetric Isotropic Turbo spin echo Acquisition (VISTA) within one scan and verified its feasibility in phantom and healthy subjects.Methods
MR Protocol: All images were obtained on a 3.0T MR scanner (Philips Achieva, Best, Netherlands). Conventional T1- and T2-weighted spin echo (SE) sequences were used to acquired reference images. Imaging parameters were: FOV = 200 x 180 x 120 mm3, spatial resolution = 0.9 x 1.2 x 4 mm3. For T1-SE, TR/TE = 600/10 ms and flip angle = 70°. For T2-SE, TR/TE = 3000/80 ms, TSE factor = 15 and flip angle = 90°. To acquire both T1- and T2-weighted images in a single scan, dual-echo with T1- and T2-weighting were generated by adjusting TR and TE values. Imaging parameters were: FOV = 200 x 180 x 120 mm3, spatial resolution = 0.6 x 0.6 x 0.6 mm3, TR = 700ms, TE (echo1/2) = 29/170 ms, TSE factor = 58 and echo spacing = 4.9 ms. After establishment of static pseudo steady state, the hard refocusing pulses were performed with reduced flip angle scheme. The refocusing flip angle and echo train length were optimized using extended phase graph4. Phantom Experiments: Cylindrical phantoms, with various portion of Gadolinium and Agar doped, were used to model signal intensity evolution of thrombus in five stages, including ‘hyperacute’, ‘acute’, ‘early subacute’, ‘late subacute’ and ‘chronic’, as reported in literature5. Signal appearance in T1 and T2-imaging were summarized in Table.1. Reference images were acquired by T1-SE and T2-SE, respectively. Dual-echo VISTA sequence was implemented to acquire T1/2 images simultaneously. Signal intensity (SI) was measured by contours at the center of each phantom. In-vivo validation: One healthy volunteer (30-year-old, male, approved by local ethics committee), with written informed consent, was scanned using dual-echo VISTA for further validation.Results
Phantom experiment results were shown in Fig.1. Signal evolution of intracranial thrombus was modeled in T1-SE and T2-SE. Echo1 and echo2, indicating T1 and T2 contrast, gained comparable signal intensity with T1/2-SE images. Signal intensity curves (Fig.2) also verified that dual-echo VISTA provided same T1/2 signal evolution information as conventional T1/2-SE sequences. Fig.3 indicated that dual-echo VISTA can provide T1- and T2-weighted images with adequate image quality, and venous sinus wall can be clearly depicted (white arrowheads).Discussion
In this study, we successfully achieved simultaneous acquisition of T1- and T2-weighted images using dual-echo VISTA, and tested its feasibility in phantom and healthy volunteers. Phantom experiments showed that dual-echo VISTA can provide T1- and T2-weighted images as conventional T1/2 imaging sequences, and the performance of proposed sequence was further validated by in-vivo scan. Dual-echo VISTA assembles flow-suppression, T1 and T2 contrast in one sequence. Benefit from the intrinsic ‘black-blood’ properties of turbo spin echo, venous sinus structures, including sinus wall, arachnoid granulations and surrounding tissues, can be adequately visualized. On the other hand, the stages of thrombus can be more accurately classified by jointly interpreting T1 and T2 images. For example, early and late subacute thrombus, both of which exhibit hyper-intense signal in T1 images, can be easily distinguished using T2 images. Furthermore, acquiring T1- and T2-images in one scan avoids inter-scan movement, which is beneficial for image analysis.Conclusion
This study demonstrated the feasibility of simultaneously acquiring T1 and T2-weighted images using dual-echo VISTA sequence. By incorporating T2 contrast, this technique has the potential to differentiate stages of thrombus more accurately.Acknowledgements
No acknowledgement found.References
1. Bousser MG, Ferro JM. Lancet Neurol. 2007;6:162–170.
2. Ferro JM, et al. Stroke. 2004;35:664–670.
3. Yang Q, et al. Stroke. 2015;47:404-409.
4. Zhou ZC, et al. JCMR 2015;17:41.
5. William GB. Radiology. 1993;189:15-26.
Figures
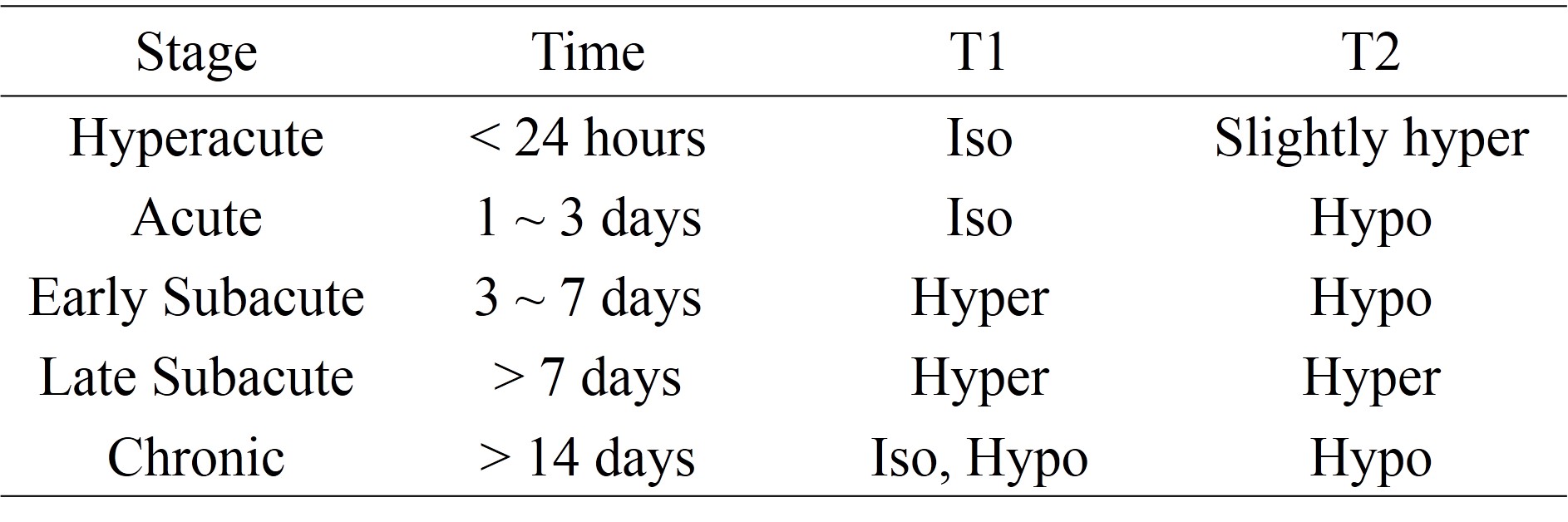
Table.1 Signal intensity evolution
of intracranial hemorrhage/thrombus in MR imaging
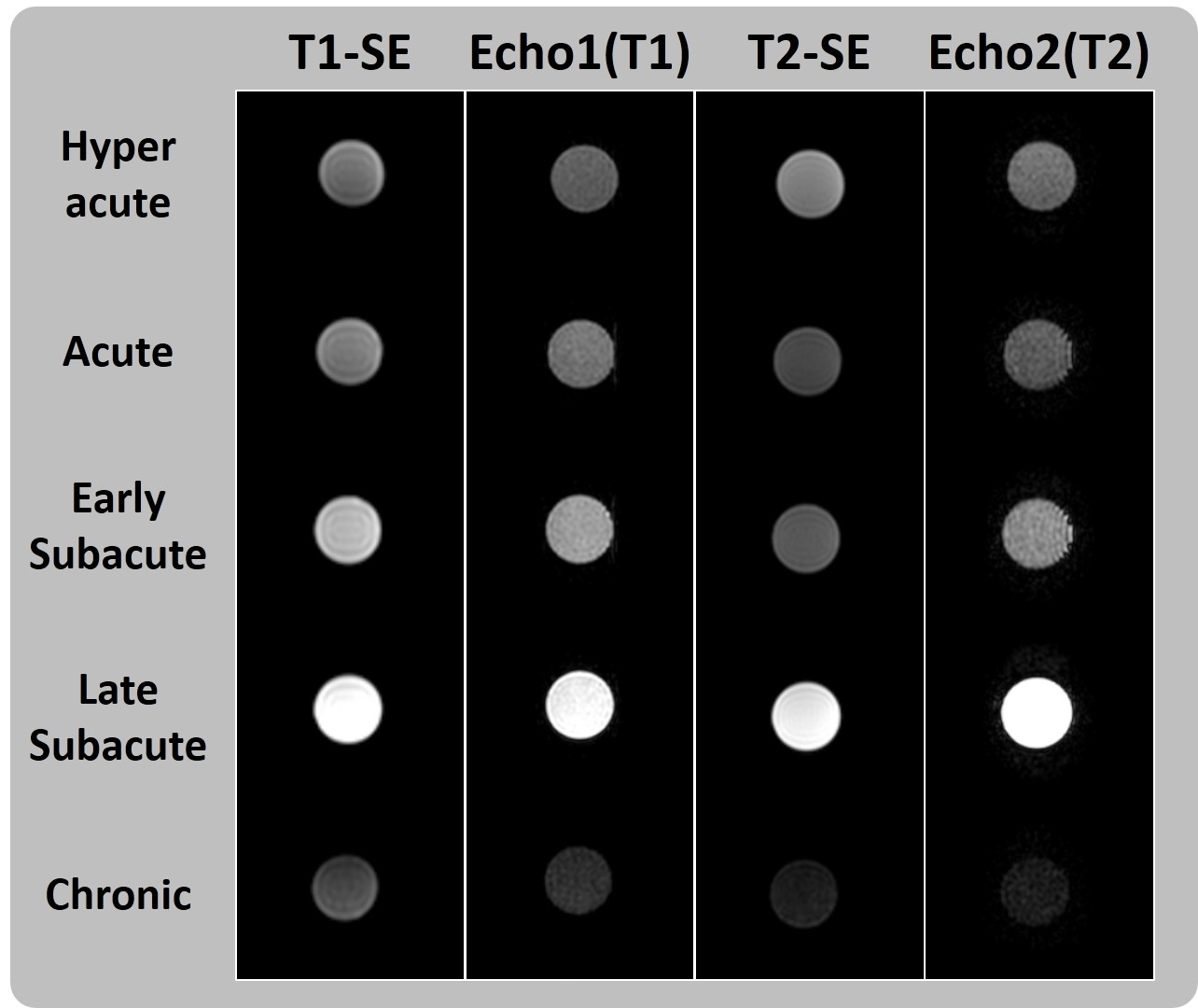
Fig.1 T1 and T2 signal intensity evolution modeled by
five cylindrical phantoms representing ‘Hyperacute’, ‘Acute’, ‘Early Subacute’,
‘Late Subacute’ and ‘Chronic’, respectively. In dual-echo VISTA sequence, T1/2
images were acquired by echo1/2.
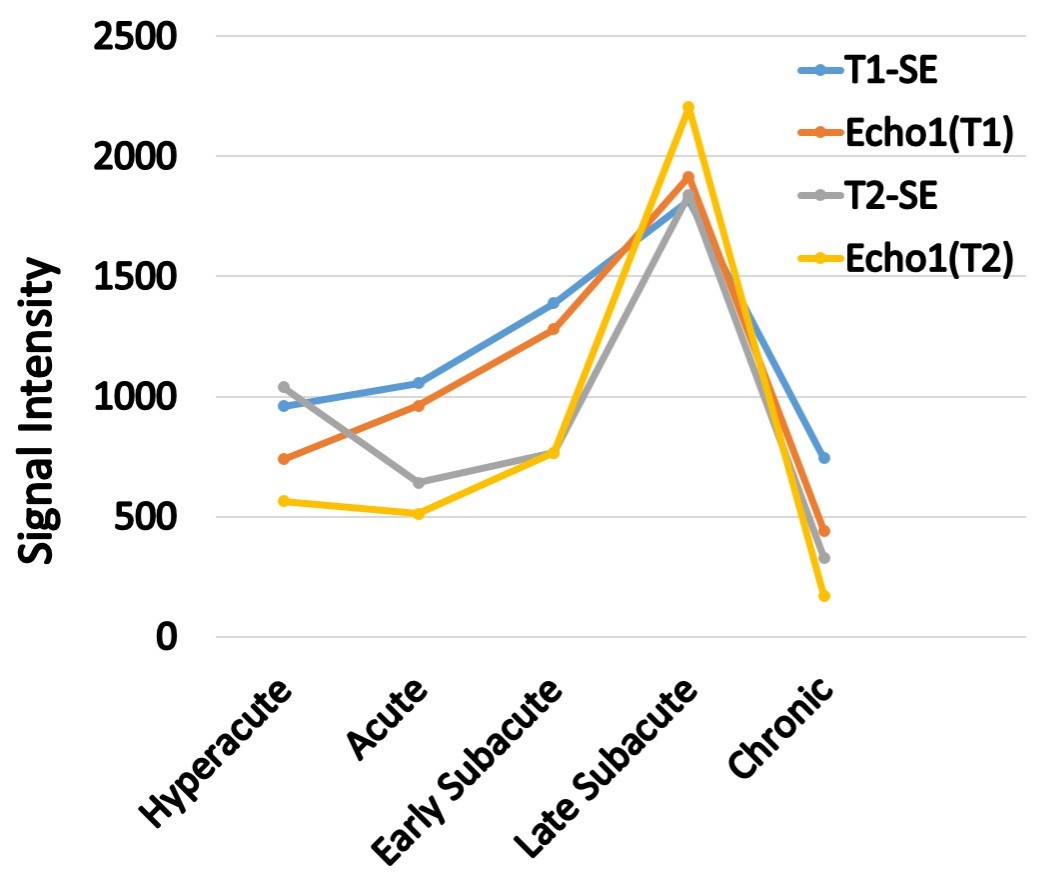
Fig.2 Signal intensity
curves of five cylindrical phantoms in T1-SE, Echo1(T1), T2-SE and Echo2(T2).
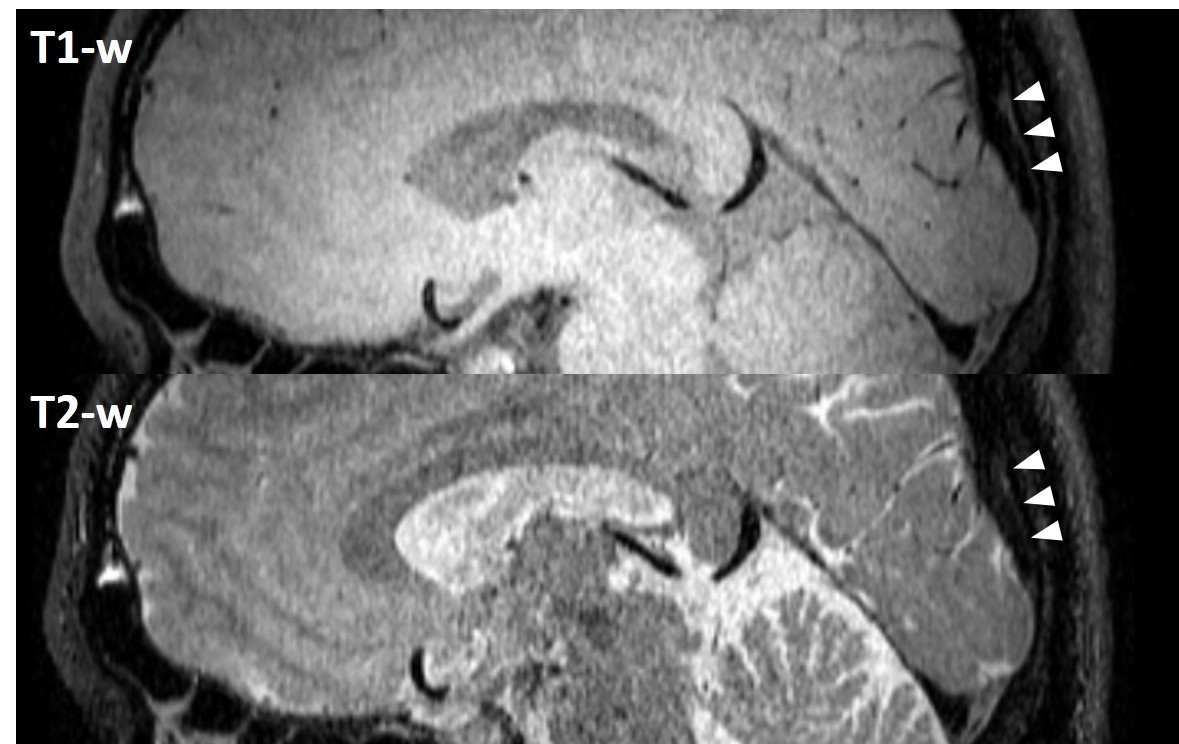
Fig.3 Dual-echo VISTA
images of a 30-year-old healthy volunteer. Blood signal was successfully
suppressed in both images and venous sinus wall were depicted (white
arrowheads).