1872
Brain Cloud of Carbogen-based Cerebrovascular Reserve : territorial and cortical specificityTzu-chen Yeh1,2, Chou-ming Cheng3, and Chi-che Chou3
1Department of Radiology, Taipei Veterans General Hospital, Taipei, Taiwan, 2Institute of Brain Science, National Yang-ming University, Taipei, Taiwan, 3Integrated Brain Research Unit, Department of Medical Research, Taipei Veterans General Hospital, Taipei, Taiwan
Synopsis
To explore the spatial characters of carbogen-based cerebrovascular reserve (CO2-CVR), grouped analyses of CO2-CVR was obtained using BOLD-based fMRI for ninety normal subjects with the fully automatic delivery system of carbogens and parametric inhalation of 1-5% CO2. Distal territories of ACA, segment 3, showed the highest of CO2-CVR at v23ab (ventral portion of Brodmann area 23) as verified by territorial and cortical parcellation. Our findings supported the biological adapation of CVR for resting activity, e.g. default mode network.
PURPOSE
Brain cloud of carbogen-based CVR (CO2-CVR) was constructed using the automatic delivery system of carbogens for parametric challenge, blood-oxygenation-level-dependence (BOLD) fMRI and database of 90 normal subjects. Territorial and cortical specificities of CO2-CVR was evaluated by regions of interest (ROI) approaches.MATERIAL AND METHODS
Whole-brain EPI (flip angle = 90 degrees, TR/TE=2000/50 msec, matrix size = 3.6x3.6x4 mm, NR=360) of normal subjects (n=120, age=20-33 years old, 66 males), was performed using a 3T MR system with recordings of end-tidal CO2 (etCO2). Data of ninety subjects (46 meles) were included by the criteria of (1) head motion (translational motion > 1 mm and rotational motion > 1 degree), (2) anatomical variant and (3) venous response of BOLD-based signal following the paradigm of carbogens. The custom-designed automatic delivery system of CO2-CVR was constructed using 1-5% CO2. Carbogen inhalation via a disposable non-rebreathing mask and a custom-designed automatic deliver system was integrated for mapping the CO2-CVR by perfusion modulation of BOLD-contrast signal. The period and concentration of carbogens were monitored by measuring the end-tidal carbon dioxide (etCO2). Carbogens (medical-graded 1-2-3-4-5% CO2, 20% O2 and 79-78-77-76-75% N2) for carbogen challenge was provided with air for control gas in high flow rate (10 liters/minute). After 130-sec baseline condition with inhalation of air, on-period of carbogen delivery and off-period of air delivery were arranged alternatively as 60-second blocks. The order of carbogens delivery is semi-randomized for each subject. The custom-designed automatic gas delivery system included implementation of hardware and software. For hardware part, six massflow devices (Vögtlin Instruments AG, Aesch, Switzerland) were integrated to control five carbogens and air, respectively. Each massflow received control of computer via RS232 port for controlling gas flow rate and duration. For software part, the user interface was constructed using Labview (National Instruments, Austin, Texas, U.S.) for controlling and monitoring massflow performance via the Labview compatible Get Red-y subroutine (Vögtlin Instruments AG, Aesch, Switzerland). For monitoring the performance of automatic delivery, on-line etCO2 measurement with gas sampling within mask was recorded for monitoring end-tidal CO2 by the Powerlab system (PowerLab TCD110 and MLT1010, ADInstruments, Castle Hill, Australia). For software part, Informax independent component analysis (ICA) was applied to obtain the CRF (carbogen response function) after preprocessing data by SPM12. And the CRF was utilized for mapping CO2-CVR of whole brain, as t values by one-sample t-test. Territorial specificities of CO2-CVR was evaluated by ROIs derived from maps of arterial transit time (https://figshare.com/articles/ATT_based_flow_territories/1488674) with three divisions of anterior cerebral arteries (ACA, 1-3 segments), middle cerebral arteries (MCA, 4-6 segments) and posterior cerebral arteries (PCA, 7-9 segments). Cortical specificities of CO2-CVR was estimated using cortical paracellation of the multimodal approach by HCP (https://figshare.com/articles/HCP_MMP1_0_projected_on_MNI2009a_GM_volumetric_in_NIfTI_format/3501911). Grouped analyses using two-sample t test were performed.RESULTS
Territorial difference of CO2-CVR showed extraordinarily low CO2-CVR in PCA (especially segment 9, p=2.4x10-6~7.9x10-19 as compared with other segments) when division 3 (distal division of ACA) had the globally highest CO2-CVR (Figure 1). Analyses of cortical parcellation showed the highest of averaged CO2-CVR as 14.5 at v23ab (ventral portion of Brodmann area 23, Figure 2).CONCLUSIONS
Territorial and cortical specificities of CO2-CVR suggested limited CO2-CVR in territories of posterior circulation and (2) vital function in distal territories of ACA as verified by cortical parcellation showing the highest of CO2-CVR at v23ab (ventral portion of Brodmann area 23). Our findings suggested the adapation of CVR for resting activity, e.g. default mode network. And “Brain Clouds” were available for users to upload raw data (contact tcyeh@vghtpe.gov.tw).Acknowledgements
Authors appreciated the support of Ministry of Science and Technology (MOST) of Taiwan (MOST 105-2221-E-075-003).References
No reference found.Figures
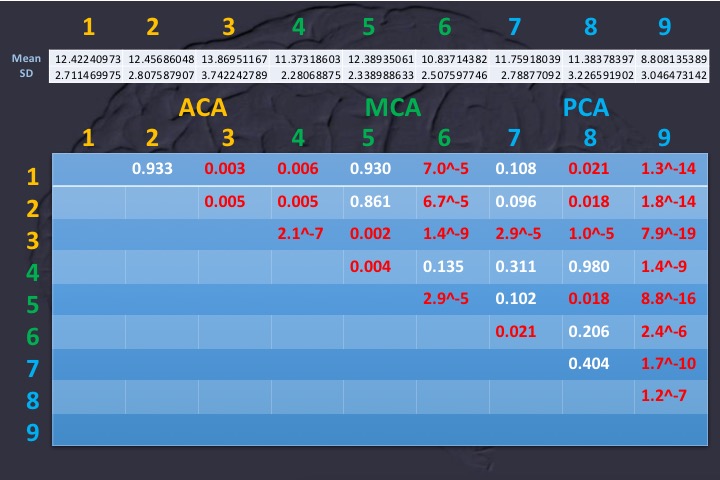
Figure 1: Averaged territorial CO2-CVR was
summarized at top table as the mean and one standard deviation for ACA (1-3
segments), MCA (4-6 segments) and PCA (7-9 segments). Comparison among segments
was demonstrated at bottom table using the two-sample tests.
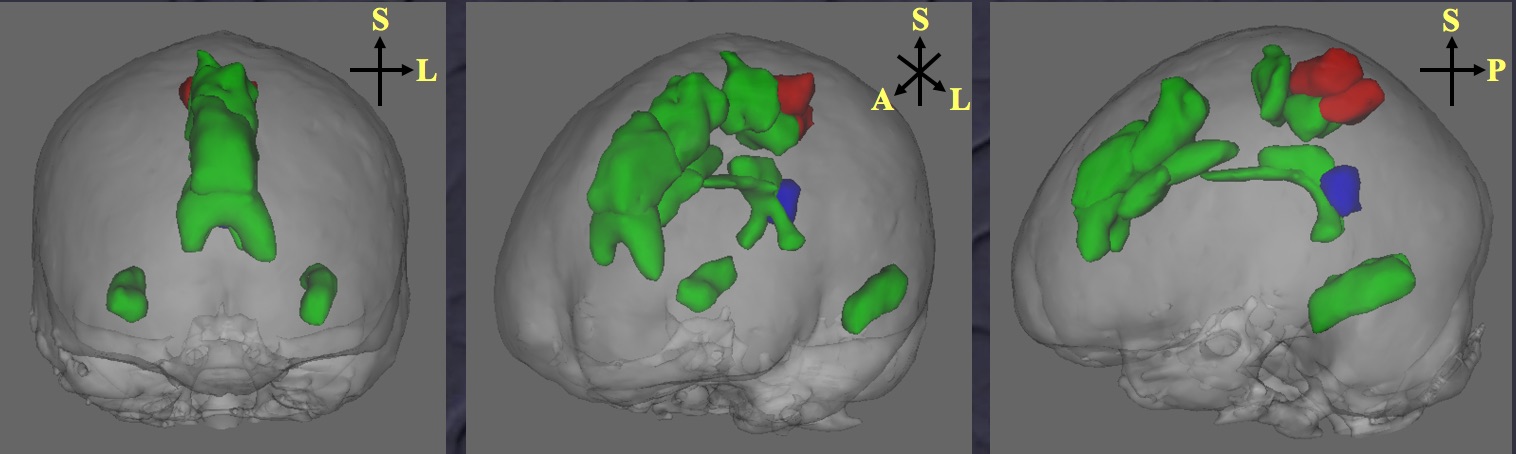
Figure 2: Highest CO2-CVR of v23ab (labeled as blue) was demonstrated by analyses of cortical parcellation. Other areas with high CO2-CVR
were labeled as red (averaged t values > 14) and green (averaged t values >
13, but < 14) areas.