1869
Increased cerebral oxygen extraction fraction measured in the ischemic stroke using an asymmetric spin echo EPI approach1GE Healthcare, Shanghai, China, 2Radiology, Huashan Hospital, Shanghai, China, 3GE Healthcare, Beijing, China
Synopsis
The oxygen consumption by brain tissue can be measured with oxygen extraction fraction (OEF), a potential indicator of the occurrence of stroke. A single shot asymmetric spin echo (ASE) EPI sequence was implemented for OEF measurement in stroke patients. Increased OEF corresponded with the decrease blood flow in the ischemic brain region, as reported in the previous literature. ASE EPI showed the potential to provide quantitative OEF maps with good brain coverage and without the need of gas challenges. The measurement of OEF may provide a better assessment of viable brain stroke after a stroke attack for potential treatment.
Purpose
Stroke is a leading cause of death and disability. The pathology, progression and treatment efficacy of stroke are extremely susceptible to status of the cerebral blood perfusion and oxygen metabolism. The oxygen consumption by brain tissue can be measured with oxygen extraction fraction (OEF), also a potential indicator of the occurrence of stroke.1 Positron emission tomography (PET) is regarded as the golden standard for OEF quantification, which involves the radiation induced side effect. Some other methods require hypercapnic and hypoxic gas challenges, which are not very practical in a clinical setting.2 Recently, a single shot asymmetric spin echo (ASE) EPI approach was reported by H. An and W. Lin for quantitative OEF measurement.3 In this study, we developed an ASE EPI sequence for measuring the OEF in the brain and performed the preliminary study on stroke patients. The measurement of OEF may provide a better assessment of viable brain stroke after a stroke attack for potential treatment.
Methods
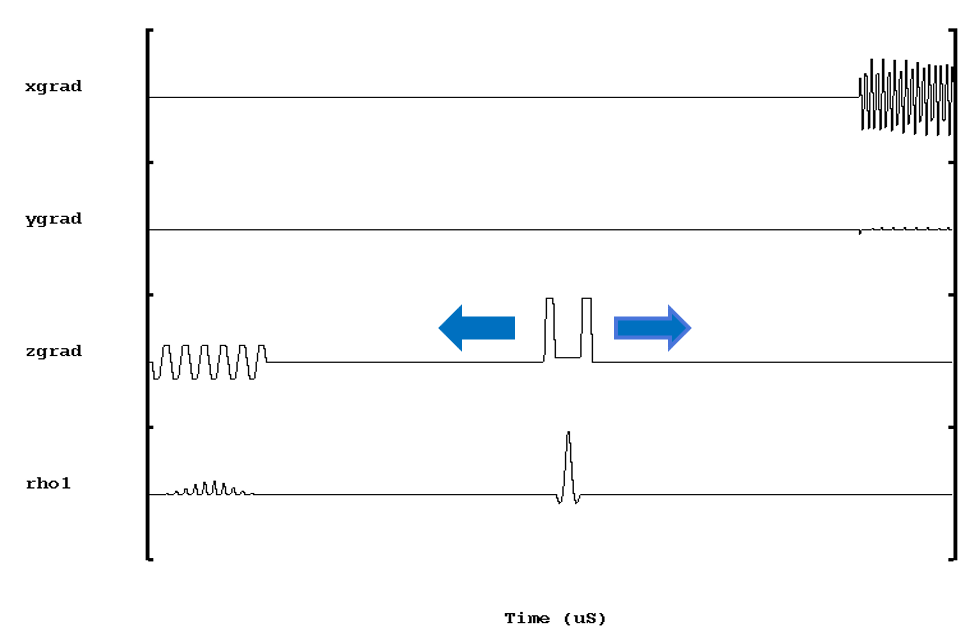
Three stroke patients (age 50-69 years old, one female) gave written informed consent to participate the study. All MRI scans were performed on a 3.0-T MR750 scanner (GE Healthcare, Milwaukee, USA) using an 8-channel phase array head coil. The ASE EPI sequence was a variation of a single-shot spin echo EPI sequence. The 180° refocusing pulse was shifted relative to the original position (time shift τ) while the time of echo (TE) was kept constant (Fig. 1). The ASE-EPI sequence used a fixed TE to achieve the same R2 weighting but various time shift τ to introduce different R2’ and R2* weighting on the acquired images. Scan parameters were as follows: TR/TE=2000/80ms, FOV=240mm, slice thickness/gap=5/1mm, acquisition matrix=64×64, number of excitations (NEX) = 3. The ASE EPI sequence was repeated 19 times to acquire 19 asymmetric spin echoes with time shift τ corresponding to -18, -16, …, 2, 0, 2, …, 16, 18ms. The total acquisition time was 4min to acquire 28 slices. The ASE EPI images were used to estimate two parameters (reciprocal of reversible transverse relaxation rate R2’ and deoxygenated blood volume λ) by fitting them to the model proposed by Haacke and Yablonskiy.4 Then δω map could be calculated using: 𝛿𝜔=𝑅2′/λ(Eq.1). After that, OEF value was estimated using the following equation: 𝑂𝐸𝐹=𝛿𝜔/(𝛾∙4/3𝜋∙∆χ∙𝐻𝑐𝑡∙𝐵0) (Eq.2), where γ was the gyromagnetic ratio, Δχ represented the susceptibility difference between fully deoxygenated blood and fully oxygenated blood with the value of 0.18ppm. Hct was the hematocrit value, which was assumed to be 0.42. The 3D arterial spin labeling technique (3DASL) was also used to acquired perfusion weighted images of stroke patients for comparison.
Results
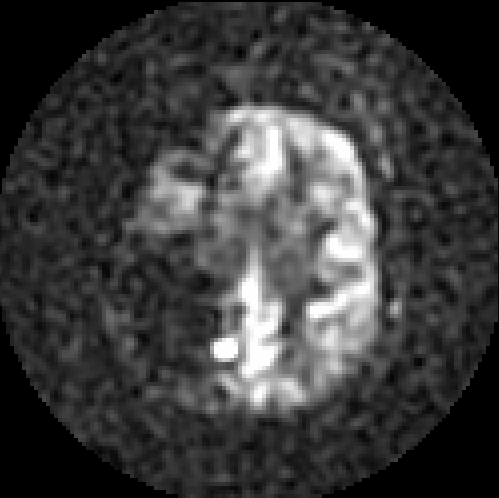
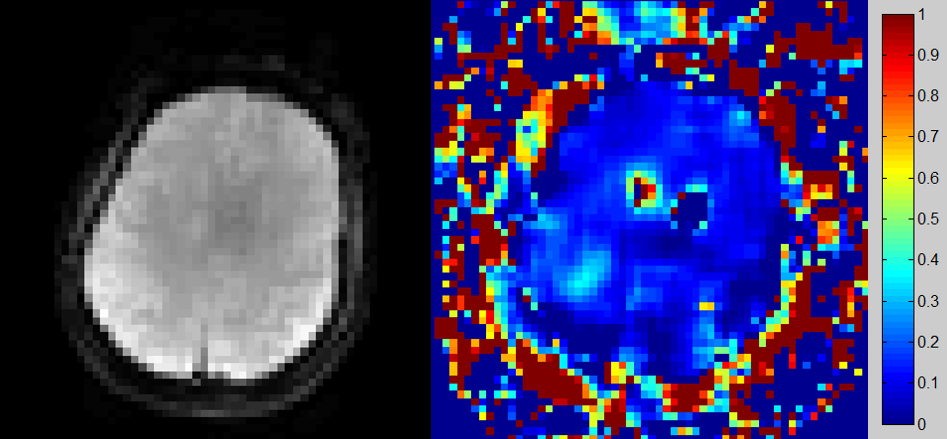
Fig.2 shows the 3DASL perfusion weighted image for a typical stroke patient with the ischemic region at the right side of the brain. The decreased cerebral blood flow was apparent as compared to the surrounding normal brain regions. Fig. 3 shows the original ASE EPI images and the calculated OEF maps of the same stroke patient. We can observe that the increased OEF corresponds with the decrease blood flow in the ischemic region in the brain, as reported in the previous literature.1
Discussion and Conclusion
ASE EPI has the potential to provide quantitative OEF maps with good brain coverage and without the need of gas challenges. These results hold promise for some clinical uses, such as stroke, showing increased OEF in the ischemic brain region with decreased blood supply. Further investigation can be extended to assess the sensitivity of OEF measurement in other disease situations such as brain tumor.Acknowledgements
No acknowledgement found.References
1. Derdeyn CP, Yundt KD, Videen TO, et al. Increased oxygen extraction fraction is associated with prior ischemic events in patients with carotid occlusion. Stroke. 1998; 29:754-758.
2. Ni WW, Christen T, Zaharchuk G. Assessing reproducibility and changes in oxygenation with R2’ during clinical hypercapnic and hypoxic gas challenges. Proc Intl Soc Mag Reson Med. 2015;1450.
3. An H, Lin W. Impact of intravascular signal on quantitative measures of cerebral oxygen extraction and blood volume under normo- and hypercapnic conditions using an asymmetric spin echo approach. Magn Reson Med. 2003;50:708–716.
4. Yablonskiy DA, Haacke EM. Theory of NMR signal behavior in magnetically inhomogeneous tissues: the static dephasing regime. Magn Reson Med. 1994;32:749–763.
Figures