1801
Factor analysis to determine white matter injury patterns following pediatric traumatic brain injury.1Radiology, Loma Linda University Medical Center, Loma Linda, CA, United States, 2Pediatrics, Loma Linda University Medical Center, Loma Linda, CA, United States
Synopsis
Several studies have shown regional disruptions in white matter integrity following TBI although conventional methods don't account for the relationship between regions. In this study we used factor analysis, a data reduction technique, to identify patterns of WM injury that are associated with neurocognitive outcome in pediatric TBI patients. Our findings identified 3 dominant patterns of WM injury in pediatric TBI patients, describing regional changes in: 1) subcortical + cortical diffusivity, 2) subcortical diffusivity, and 3) subcortical + cortical anisotropy. Factor analysis provides a unique statistical approach to analyze DTI data and potentially could be used to combine different data streams (DTI, MR spectroscopy, SWI) representing different elements of injury.
Purpose
Traumatic brain injury (TBI) is associated with widespread disruption in white matter (WM) integrity. DTI studies of pediatric TBI patients have shown regional changes in fractional anisotropy (FA) and apparent diffusion coefficient (ADC)/mean diffusivity (MD) that suggest evolving axonal and myelin injury1. Conventional analytical methods (TBSS or region of interest analysis) identify brain regions in which DTI metrics differ among groups; however the relations between brain regions is not taken into account. Factor analysis is a data reduction technique that can condense a large number of variables into clusters of correlated variables (factors). The purpose of our study was to use factor analysis to identify patterns of WM injury (DTI metric and/or region) that are associated with neurocognitive outcome in pediatric TBI patients.Methods
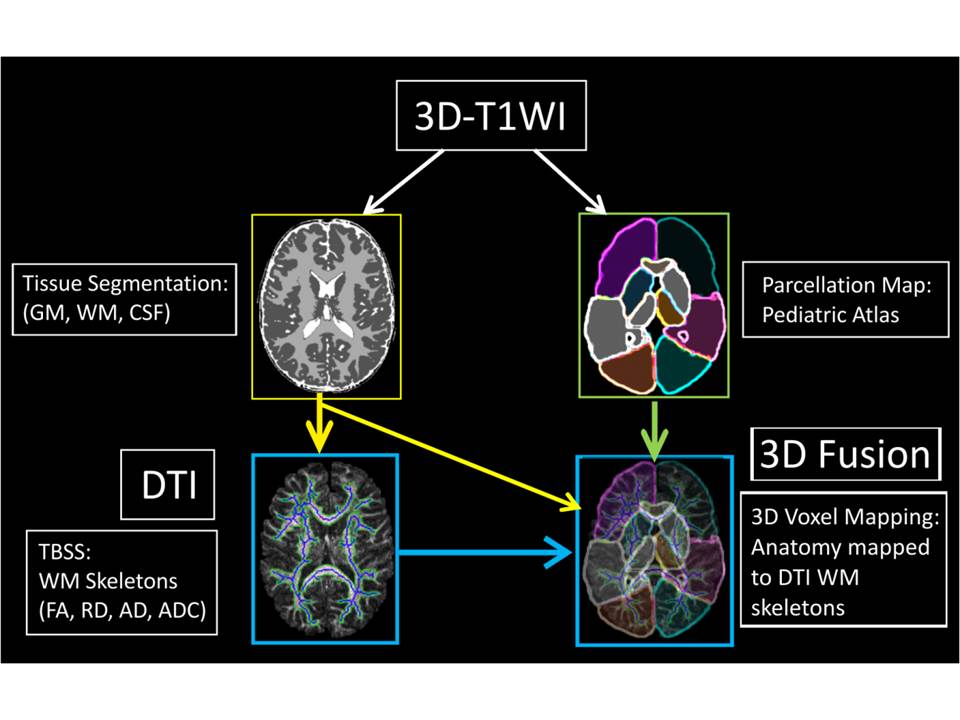
Pediatric subjects who sustained a complicated mild/moderate (n = 10, mean age = 12 ± 4 years) or severe (n = 18, age = 12 ± 4 years) TBI were studied. A cohort of healthy adolescents (n = 37, mean age = 14 ± 3 years) were enrolled as controls. Conventional 3D T1 weighted (T1WI, MPRAGE, repetition time (TR) and echo time (TE) = 1950 ms and 2.26 ms, 1.0 x 1.0 x 1.0 pixel size) and 30 direction DTI (TR/TE = 5700/1022 ms, 1.2 x 1.2 x 3.0 pixel size, 0.9 mm gap, b = 0 and 1000 s/mm2) were acquired using a 3T Siemens Tim Trio MR scanner equipped with a 12 channel receive-only head coil. Patients were imaged within 6-17 days post injury. DTI data were preprocessed (interpolation to meet the resolution of the T1 MPRAGE images, skull stripping, and CSF masking) and DTI maps were computed using tract-based spatial statistics (TBSS) according to the method of Ghosh et al2. Anatomic regions were acquired from the T1WI and co-registered DTI data using a pediatric brain parsing pipeline from the Laboratory of Neuroimaging (LONI) Brain Parser software catalog (University of Southern California, CA; http:// www.pipeline.loni.usc.edu, Fig 1).
Cognitive and neurological testing at 1 year after injury included the Wechsler Abbreviated Scale of Intelligence (FSIQ), Performance Intelligence Quotient (PIQ), verbal intelligence quotient (VIQ), the Test of Everyday Attention - Children (TEACH G and C), children’s memory scale (CMS), and pediatric cerebral performance category scale (PCPCS). Between group differences in regional DTI metrics were determined using a Kruskal Wallace one-way ANOVA with Bonferroni post-hoc analysis.
Factor analysis of the DTI metrics from individual cortical and subcortical regions was performed using the method of Mohamed et al3. Spearman rank correlations were used to relate neurocognitive test scores with the imaging factors. Statistical analyses were performed in SPSS (version 22; Chicago, USA) and findings considered significant when p < 0.05.
Results
Compared to controls, FA was reduced in the basal ganglia, corpus callosum, occipital and parietal white matter regions of severe TBI patients (p ≤ 0.001). Factor analysis of the regional DTI metrics identified 6 factors, accounting for 87.7% of the variance in the original data set. Factor 1, accounting for 45.2% of the variance, included ADC, axial diffusivity (AD), and radial diffusivity (RD) measurements from basal ganglia, corpus callosum, frontal, parietal, temporal and occipital WM regions. Factor 2 (13.9% of the variance) included ADC, AD, and RD measurements from basal ganglia, brainstem, corpus callosum, and thalami. Factor 3 (10.5% of the variance) included the mean FA of basal ganglia, brainstem, cerebellum, frontal, parietal, temporal and occipital WM regions. Only factor 1 showed significant association with 12-month neurocognitive testing: PIQ (r = .506 p = .007) and FSIQ (r = .427 p = .026).Discussion
Our findings show that factor analysis of DTI identified 3 dominant patterns of WM injury in pediatric TBI patients, describing regional changes in: 1) subcortical + cortical diffusivity (ADC, RD, AD), 2) subcortical diffusivity, and 3) subcortical + cortical anisotropy (FA). Unlike prior studies showing a relationship between FA and outcome, our study showed that only subcortical + cortical diffusivity was associated with 12 month neurocognitive outcomes. Factor analysis provides a unique statistical approach to analyze DTI data and potentially could be used to combine different data streams (DTI, MR spectroscopy, SWI) representing different elements of injury.Acknowledgements
Supported by the NINDS R01-NS054001References
1. Roberts RM, Mathias JL, Rose SE. Relationship Between Diffusion Tensor Imaging (DTI) Findings and Cognition Following Pediatric TBI: A Meta-Analytic Review. Dev Neuropsychol. 2016 Apr;41(3):176-200.
2. Ghosh N, Holshouser B, Oyoyo U, Barnes S, Tong K, Ashwal S. Combined Diffusion Tensor and Magnetic Resonance Spectroscopic Imaging Methodology for Automated Regional Brain Analysis: Application in a Normal Pediatric Population. Dev Neurosci. 2017;39(5):413-429.
3. Mohamed MA, Lentz MR, Lee V, Halpern EF, Sacktor N, Selnes O, Barker PB, Pomper MG. Factor analysis of proton MR spectroscopic imaging data in HIV infection: metabolite-derived factors help identify infection and dementia. Radiology. 2010 Feb;254(2):577-86.
Figures