1800
Tag-Based CSF Imaging Performance in Pediatric Patients and Adult Volunteers1Center for Fetal and Neonatal Medicine, Division of Neonatology | Children's Hospital Los Angeles, Department of Pediatrics, Keck School of Medicine, University of Southern California, Los Angeles, CA, Los Angeles, CA, United States, 2USC/LAC+USC Neonatal-Perinatal Medicine Fellowship Program, Division of Neonatology LAC+USC Medical Center & Children’s Hospital Los Angeles, Keck School of Medicine of USC, Los Angeles, CA, Los Angeles, CA, United States, 3Department of Radiology, Children’s Hospital Los Angeles, Los Angeles, CA, Los Angeles, CA, United States, 4Rudi Schulte Research Institute, Santa Barbara, CA, Santa Barbara, CA, United States, 5Department of Radiology, Keck School of Medicine, University of Southern California, Los Angeles, CA, Los Angeles, CA, United States, 6Department of Radiology, University of California San Diego, La Jolla, CA, La Jolla, CA, United States, 7Division of Neurosurgery, Children’s Hospital Los Angeles, Los Angeles, CA, Los Angeles, CA, United States, 8Department of Neurological Surgery, Keck School of Medicine, University of Southern California, Los Angeles CA, Los Angeles, CA, United States
Synopsis
We compared tag-based CSF imaging techniques (TimeSLIP and TimeSTAMP) in 10 healthy adults and 19 pediatric patients with cerebrospinal fluid (CSF) abnormalities. In adults, TimeSLIP and TimeSTAMP contrasts were quantitatively compared. TimeSTAMP sequences showed higher contrasts with decreased contrast variability versus TimeSLIP sequences. In pediatric patients, TimeSTAMP sequences were acquired to observe clinical utility and had
Introduction
Advanced magnetic resonance imaging sequences are used to study cerebrospinal fluid (CSF) flow physiology and alterations in varying central nervous system disorders.1 CSF flow disorders, particularly hydrocephalus, may benefit from clinical applications of these sequences. Time-Spatial Labeling Inversion Pulse (TimeSLIP) uses an arterial spin labeling technique to tag CSF as an endogenous tracer: one non-selective 180-degree pulse suppresses the stationary tissue signal and a second 180-degree to create the bright CSF as a tracer. A series of single-shot images with incremental inversion recovery delay times (TD) then capture CSF flow.2 However with TimeSLIP, changes in the background signal may render image interpretation more difficult. We used a variant of tag-based flow imaging called Time Static Tagging And Mono-contrast Preservation (TimeSTAMP), that minimizes the changing contrasts to improve image quality. We acquired TimeSLIP and TimeSTAMP images healthy adults to compare their contrasts, and TimeSTAMP in pediatric patients to explore clinical applicability.Methods
Subjects: Ten healthy adults (5 male, 5 female, 36 ± 18 years) were recruited and had both TimeSLIP and TimeSTAMP images acquired. Nineteen pediatric patients (12 male, 7 female, 1 month to 13 years) with CSF abnormalities had TimeSTAMP images acquired. Abnormalities were mainly congenital and acquired hydrocephalus requiring surgical intervention; etiologies included tumors, arachnoid cysts and webs, post-hemorrhagic changes and structural malformations.
Acquisition: Two clinical 3T MR scanners were used for healthy adults (Titan 3T, Toshiba, Toshiba American Medical Systems, Irvine, CA), and pediatric patients (Achieva Philips, Best, the Netherlands). Both tag-based sequences used similar half-fourier fast spin echo readouts. The image parameters for adults were (TE=80ms, TR=13450ms, FA=90 degrees, acquisition matrix 224x224, voxel resolution=1.0x1.0x5.0mm3). The parameters for pediatric patients were (TE=7ms, TR=8000ms, FA=70 degrees, acquisition matrix 256x161, voxel resolution=0.9x1.4x4.0mm3).For TimeSLIP, twenty cardiac-gated images were acquired at TDs of 1700 to 3700ms. For TimeSTAMP, gating was omitted and images were acquired at nearly constant delay times. TimeSTAMP sequences differed slightly for adults (20 dynamics, TD≈2700ms and pediatric patients (typically 9 dynamics, TD=2500ms).
Image Review: Images were analyzed in Matlab (Mathworks Natick, MA). For healthy adults, ROIs were parenchyma (brainstem), tagged CSF (fourth ventricle) untagged CSF (lateral ventricle) and flowing CSF (third ventricle and aqueduct). Pediatric patient pathology caused various tag placements. CSF ROIs included the lateral, third, and fourth ventricles, pre-pontine and interpeduncular cistern and cisterna magna.
Results
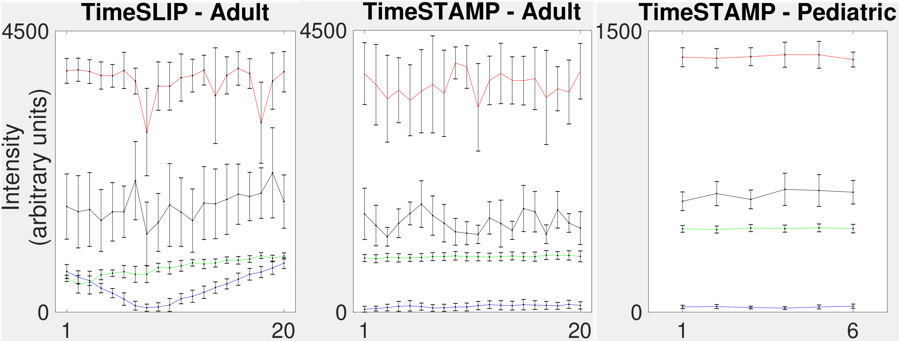
Representative TimeSLIP and TimeSTAMP images from one healthy adult, and TimeSTAMP images from one pediatric patient demonstrate CSF flow and image contrast (Figure 1). The image-by-image ROI intensities for these cases are shown (Figure 2). As expected, there were larger fluctuations in image contrast for TimeSLIP images than for TimeSTAMP images.The greatest improvement in contrast due to TimeSTAMP happened between was between the paranchyma and untagged CSF, where the TimeSTAMP contrast was 14000 ± 1500 approximately 38% higher than TimeSLIP contrast of 9800 ± 1500. Values reported mean ± standard deviation in arbitrary units. A two-way ANOVA indicated sequence-to-sequence changes were significant (p<0.0001), even after removing the significant (p<0.0001) patient-to-patient variability in contrast. In pediatric patients, the TimeSTAMP contrast for tagged and untagged CSF was 3900 ± 1500.
Discussion
Untagged CSF in TimeSTAMP has nearly constant delay time and hence less variable contrast as demonstrated in healthy adults. Contrasts of paired ROIs in the pediatric patients showed similar performance.
TimeSLIP has been previously used to study the physiology of CSF flow in adult patients, with particular application to image hydrocephalus2-4 and observe changes following surgical interventions. However, infants undergoing surgical evaluation for CSF abnormalities have not been previously studied with tag-based CSF imaging techniques. TimeSTAMP may offer improved clinical visualization of CSF flow abnormalities in these patients. Further pediatric studies will seek to elucidate contributing factors, i.e. impedance of flows or failure of CSF reabsorption, or provide imaging characteristics relating to the timing of surgical interventions
Conclusion
TimeSTAMP has better image contrast than TimeSLIP as demonstrated in adult subjects. Pediatric patients have similar performance. Therefore, TimeSTAMP may be a superior imaging technique to observe CSF flow in patients with suspected abnormalities.Acknowledgements
Thank you to the Rudi Schulte Research Institute for supporting our reserach.References
1. Yamada S, Tsuchiya K, Bradley WG, Law M, Winkler ML, Borzage MT, Miyazaki M, Kelly EJ, McComb JG. Current and Emerging MR Imaging Techniques for the Diagnosis and Management of CSF Flow Disorders: A Review of Phase-Contrast and Time-Spatial Labeling Inversion Pulse. Am J Neuroradiol 2015;36:623-30. doi: 10.3174/ajnr.A4030.
2. Kelly EJ, Yamada S. Cerebrospinal Fluid Flow Studies and Recent Advancements. Semin Ultrasound CT MRI 2016;37:9299. doi: 10.1053/j.sult.2016.01.002.
3. Yamada S, Miyazaki M, Kanazawa H, Higashi M, Morohoshi Y, Bluml S, McComb JG. Visualization of Cerebrospinal Fluid Movement with Spin Labeling at MR Imaging: Preliminary Results in Normal and Pathophysiologic Conditions. Radiology 2008;249:644–652. doi: 10.1148/radiol.2492071985.
4. Abe K, Ono Y, Yoneyama H et al. Assessment of Cerebrospinal Fluid Flow Patterns Using the Time-Spatial Labeling Inversion Pulse Technique with 3T MRI: Early Clinical Experiences. The Neuroradiology Journal. 2014;27(3):268-279. doi: 10.15274/nrj-2014-10045.
Figures