1771
Automatic Brain Segmentation in a Neonatal Population Using a Multi-Delay Multi-Echo Sequence1Department of Radiology, Vrije Universiteit Brussel (VUB), Universitair Ziekenhuis Brussel (UZ Brussel), Brussels, Belgium, 2SyntheticMR AB, Linköping, Sweden
Synopsis
Synthetic MRI using a multi-delay multi-echo sequence was applied to a pre-term neonatal and
Introduction
The development of the young human brain is accompanied by fast changes both in brain structure and tissue characteristics during the first few years. Neonates, in particular, are liable to suffer from developmental disorders in this process, and detecting risk factors for these disorders could help in determining further follow up. Recently a multi-delay multi-echo sequence has allowed for a fast, fully automatic segmentation of the brain. This technique was applied to a group of full-term and preterm neonates, and the relation between various volumetric brain development parameters and either gestational age for the preterm patients, or corrected age for the whole population, was investigated.Methods
31 preterm born neonates (born 205 ± 19 days gestational age, 14 females) were scanned near term equivalent age. 13 full term born neonates and infants were scanned at various times after birth (mean age 29 +/- 32 days, 7 females). All scans were performed on a 3T Philips Achieva, using a multi-delay multi-echo sequence with four saturation delays, two echo times and a TR of 5000ms. FOV was 180 x 130 mm with an acquisition resolution of 0.7x0.9 mm; 30 slices were acquired with a 3.0 mm thickness and 0,3mm gap, the timing was 6min10s. Additionally, a 3D T1 weighted and a 3D T2 weighted TSE sequence image were acquired.
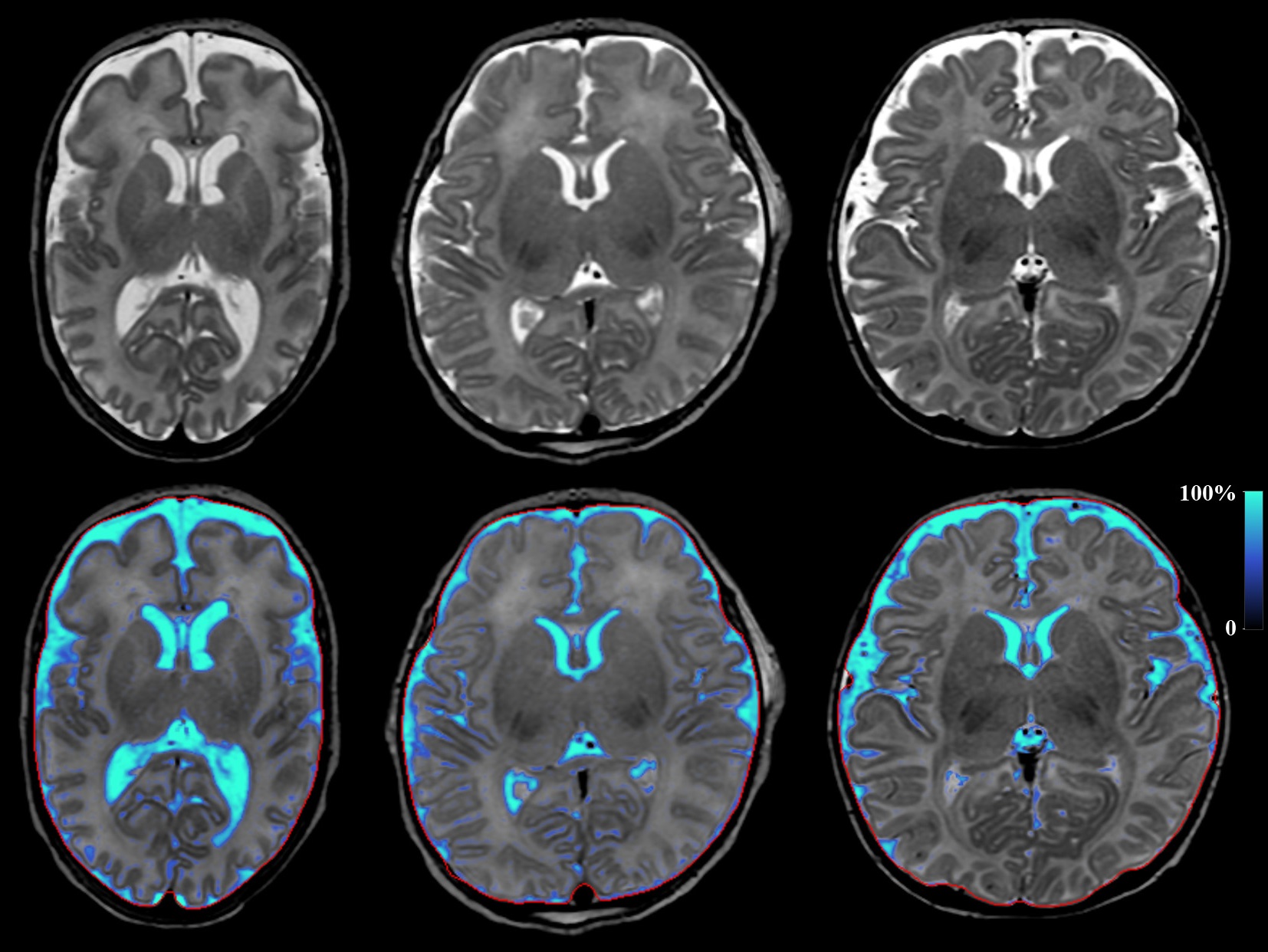
The data was analyzed and segmented using an adapted version of SyMRI 8 where detected CSF partial volume in neonates was suppressed (SyntheticMR, Linköping, Sweden). The R1 and R2 relaxation rates and proton-density parameter maps are estimated, and the brain is segmented into different tissues based on a look-up table in a three-dimensional space 1. After segmentation, the intra-cranial volume (ICV), Brain Parenchymal Volume (BPV) and Fraction (BPF) are also calculated, as well as the GM, WM, and CSF fractions.
For the preterm neonates, Kidokoro’s score was calculated using the 3D scans by a trained neonatal neuroradiologist. During scoring the severity of brain development impairment is scored by manually measuring landmarks and counting lesions ².
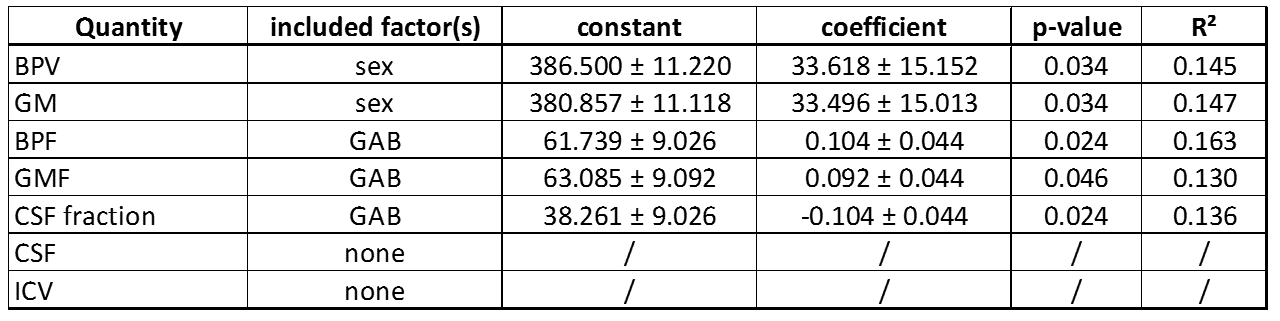
To investigate whether the gestational age at birth (GAB) affected brain measures, a linear regression was performed using SPSS 23 (IBM, Armonk, NY, USA) for the absolute BPV, GM, CSF, ICV and for the relative fractions BPF, GMF and CSF. Both sex and GAB were added stepwise as factors in the model.
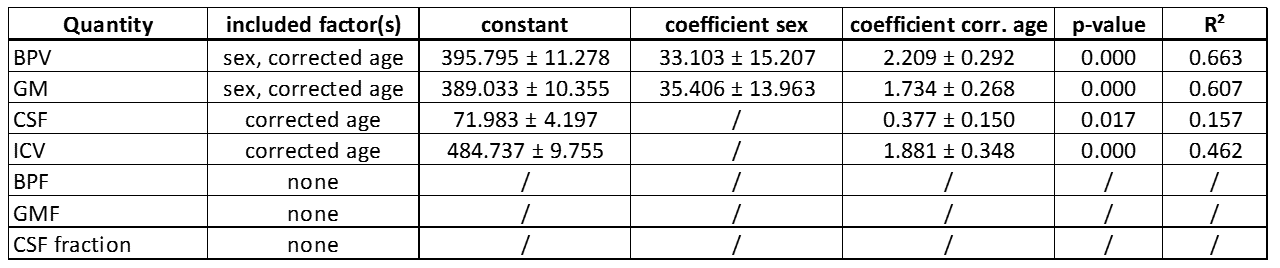
Additionally, the preterm neonates with a normal Kidokoro score (<4) and the term born children (total n=37) were analyzed to investigate the development of the brain, by performing a linear regression on the same volumetric parameters as above, with corrected age and sex as factors in the regression. The preterm children were only included if the preterm analysis found no connection between GAB and the parameter under investigation.
Results
An example of the fully automatic brain segmentation for children scanned at different ages is provided in figure 1. The results of the linear regressions on the preterm population are presented in table 1. Excluding children with an abnormal Kidokoro’s score did not change the significance of the regression results. The regression results for all neonates are presented in table 2. For the absolute volumes, the preterm population was included, as no statistical difference was found in the previous tests, with the corrected age (days) = GAB–280+age at time of scanning.
Discussion
To our knowledge, this is the first work where this method is applied to a neonatal population, although work in older children has been published recently 3. An important limitation of the current method in neonates is that most brain matter is recognized as grey matter, as GM and WM have not yet developed enough to be readily distinguishable, leading to a very high correlation between GM and BPV. However, the BPV and CSF are estimated reliably and can be used to follow the brain maturation in a term population. Previously the immature brain was identified as having a significant fraction of CSF. It was found that the BPF, GMF and CSF fraction were dependent on GAB, with the higher BPF and GMF resulting in a lower CSF fraction for children born closer to term date. The exact clinical implication of this finding cannot yet be determined, but it might indicate that a lower GAB has measurable effects on brain development.Conclusion
Neonatal BPV and BPF, intra-cranial volume, and CSF volume and fraction can be obtained reliably using a multi-delay multi-echo sequence and a relaxation parameters based segmentation algorithm. Development at a young age can be characterized, as well as differences in development in a pre-term born population.Acknowledgements
References
1. West J, Warntjes JB, Lundberg P. Novel whole brain segmentation and volume estimation using quantitative MRI. Eur Radiol. 2012 May;22(5):998-1007. doi: 10.1007/s00330-011-2336-7
2. Kidokoro H, Neil J, Inder T. A New MRI Assessment Tool to Define Brain Abnormalities in Very Preterm Infants at Term, AJNR Am J Neuroradiol. 2013 Nov-Dec; 34(11): 2208–2214. doi: 10.3174/ajnr.A3521
3. McAllister A, Leach J, West H, Jones B, Zhang B, Serai S. Quantitative Synthetic MRI in Children: Normative Intracranial Tissue Segmentation Values during Development. AJNR Am J Neuroradiol. 2017 Oct 5. doi: 10.3174/ajnr.A5398
Figures