1700
A 22-Channel RF coil array for fetus MR imaging at 3TChao Luo1,2, Guoxi Xie3, Jo Lee1,2, Xing Yang4, Xiaoliang Zhang5,6, Xin Liu1,2, and Ye Li1,2
1Lauterbur Research Center for Biomedical Imaging, Shenzhen Institutes of Advanced Technology, Chinese Academy of Sciences, Shenzhen, China, 2Shenzhen Key Laboratory for MRI, Shenzhen, China, 3School of Basic Science, Guangzhou Medical University, Guangzhou, China, 4High-Field Magnetic Resonance Brain Imaging Key Laboratory of Sichuan Province, Chengdu, China, 5Department of Radiology and Biomedical Imaging, University of California San Francisco, San Francisco, CA, United States, 6UCSF/UC Berkeley Joint Graduate Group in Bioengineering, San Francisco, CA, United States
Synopsis
Due to lack of dedicated fetal imaging RF coils, the system body coil is often used to acquire fetal images. This setup is not optimized and offers limited sensitivity and image quality. In this work, we designed and manufactured a 22-channel flexible coil array for fetal examinations. Compared with Siemens 6-channel body coil, the proposed fetal coil array achieves significant improvements in imaging coverage, image SNR and parallel acceleration capability.
Introduction
MRI is advantageous in fetal imaging due to its high soft-tissue contrast, high resolution, and dynamic imaging capability., and has become an important prenatal supplementary examination1. However, owing to lack of dedicated fetal imaging RF coils, the system body coil is often used to acquire fetal images. This setup is not optimized for the fetal applications and offers limited sensitivity, parallel imaging capability2,3, and image quality. In this work, we designed and manufactured a 22-channel flexible coil array for fetal examinations. Compared with Siemens 6-channel body coil, the proposed fetal coil array achieves significant improvements in imaging coverage, image SNR and parallel acceleration capability.Methods
According to clinical requirements and anatomical structure, the proposed 22-channel fetal coil was designed at 3T with an overall size of 310×900mm2 and covered by the polyethylene material. The proposed 22-channel fetal coil consisted of twenty-two elements, as shown in Fig. 1. The width of the copper tape was 5 mm. The dimensions of the loop 1, 5, 20, 22 were 110×160mm2, and loop 2, 6, 15, 18 were 110×150mm2; and loop 8, 9, 11, 12, 14, 17 were 110×126mm2, and the rest of loop were 120×126mm2. All the loops were tuned to 123.2 MHz, corresponding to the proton Larmor frequency at 3T. The adjacent loops overlapped to minimize the coupling between loops and the average S-parameter was approximately -15 dB or less. The proposed 22-channel fetal coil array and the Siemens 6-channel body coil array were tested on Siemens trio MRI 3T scanner in phantom experiment firstly. The gradient echo (GRE) sequence with the following parameters was used to acquire the phantom images of signal: TR/TE /band width/flip angle = 300ms/10ms/130 Hz/pixel/60 degree, FOV/matrix/slice thickness = 400×400mm2/256×256/3 mm. The commercial Siemens 6-channel body coil was used as a reference with the same protocol. The covariance weighted root-sum-of-squares (Cov-rSoS) was employed to estimate the image SNR of 22-channel fetal coil and 6-channel Siemens body coil with nine elements of spine coils. Images are acquired in the transverse, sagittal and coronal planes. The HASTE sequence with the following parameters was used to acquire the fetal head images: TR/TE /band width/flip angle = 966ms/61ms /781 Hz/pixel /140 degree, FOV/matrix/slice thickness/slices/accelerate factor = 360×360mm2/256×165/3mm/31/2. The TRUFI sequence with the following parameters was used to acquire the fetal heart images4: TR/TE /band width/flip angle = 85.25ms/1.21ms/1502Hz/pixel/60 degree, FOV/matrix/slice thickness/slices/accelerate factor = 360×360mm2/208×208/4mm/1/4. In all experiments, the proposed 22-channel fetal coil and the 9-channel spine coil were combined as the receive coil. Furthermore, a high dielectric pad was placed between the back of pregnant woman and sickbed during all the fetal imaging. Furthermore, a high dielectric pad was placed between the back of pregnant woman and patient table during all the fetal imaging.Results
The Q-factors for unload/load were 127.2/11.8 which was measured with a network analyzer. The noise correlation matrix of proposed 22-channel fetal coil and 6-channel Siemens body coil was measured from noise images and shown in Fig 2. The maximal mutual coupling coefficient is less than 0.46. The coupling between the two set of the coil arrays is negligible according to the noise correlation matrix. The SNR maps of transverse profile for the proposed 22-channel fetal coil array and 6-channel body coil were demonstrated in Figure 3. Compared with Siemens 6-channel body coil, the mean of SNR at least increased by 11% in the center region of phantom. The average and maximum g-factors in the black circle are listed below the 1/g-factor maps for comparison as shown in Fig. 4. The fetal head and heart can be seen clearly from the fetal images acquired with the proposed 22-channel fetal coil array as shown in Fig. 5.Discussion/Conclusion
The comparisons between the proposed 22-channel fetal coil array and a commercial Siemens 6-channel body coil were performed in phantom experiments to validate the performance of the designed 22-channel fetal coil array. Based on the analysis of the phantom experiment, the proposed 22-channel fetal coil array was superior to the Siemens 6-channel body coil in term of SNR, longitudinal imaging coverage, penetration and parallel performance. The fetus head and heart images were obtained with the proposed 22-channel fetal coil array in clinical examination, showing its potential of the fetal coil array for the clinical diagnosis.Acknowledgements
This work was supported in part by NSFC under Grant No. 61571433, 81527901, 81527901, 81327801 and 81627901. Guangdong Province grants 2014A030313691, 2015B020214006 and 2014B030301013. Youth Innovation Promotion Association of CAS No. 2017415, city grants KQJSCX20160301143250 and JCYJ20170413161314734 and a Pengcheng Scholar Award.References
[1] Wielandner Alice, et al. Potential of magnetic resonance for imaging the fetal heart. Seminars in Fetal and Neonatal Medicine. Vol. 18. No. 5. WB Saunders, 2013. [2] Ye Li, et al. Parallel MRI performance evaluation of a novel 32 channel fetal array at 1.5T, 20th ISMRM, 2012, 0568. [3] Keil B, Wald L L. Massively parallel MRI detector arrays. Journal of magnetic resonance, 2013, 229: 75-89. [4] Yamashita, Yasuyuki, et al. MR imaging of the fetus by a HASTE sequence. American journal of roentgenology 168.2 (1997): 513-519.Figures
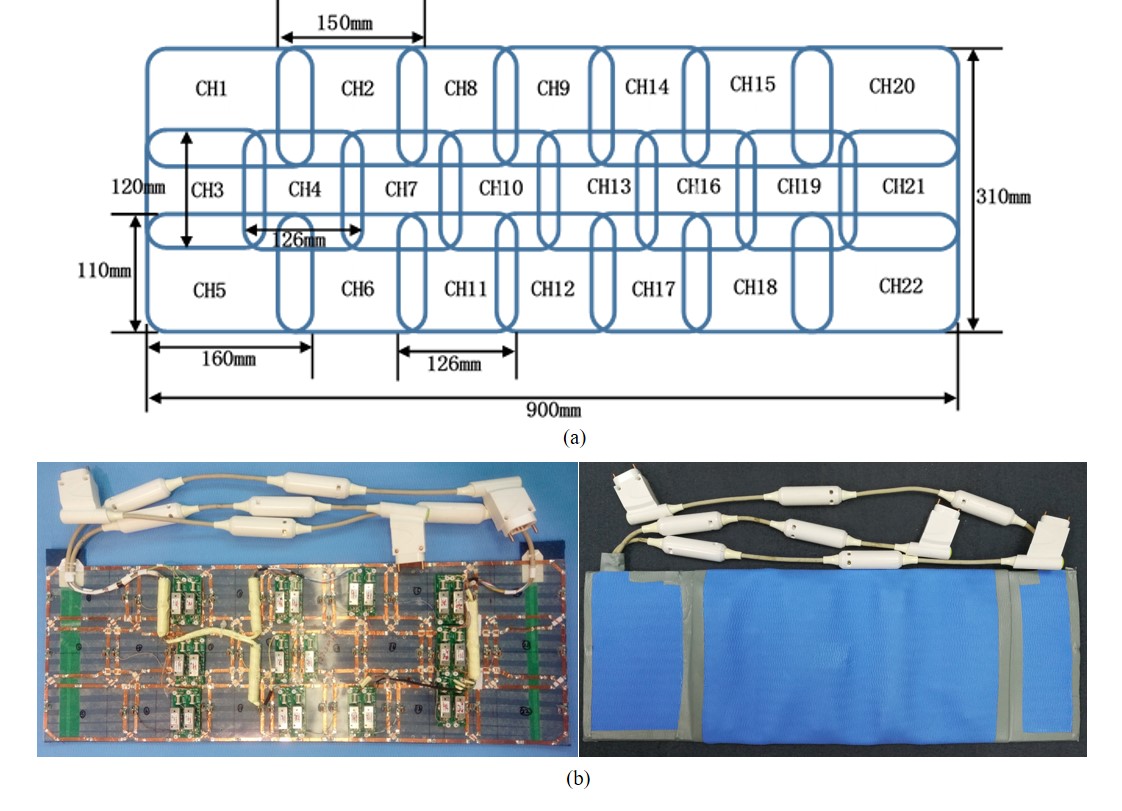
Fig. 1. (a) The layout of the
proposed 22-channel fetal coil array. (b) The fabricated 22-channel fetal coil.
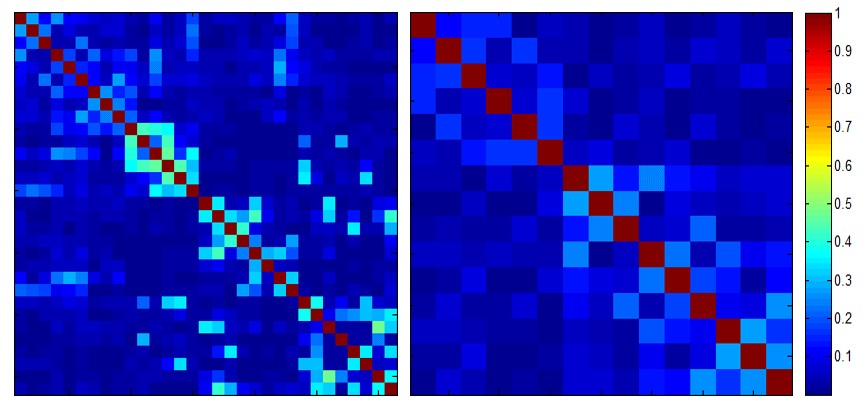
Fig. 2. The noise correlation
matrix of the proposed 22-channel fetal coil with nine elements of the spine
coil array (left) and the 6-channel Siemens body coil with nine elements of the
spine coil array (right).
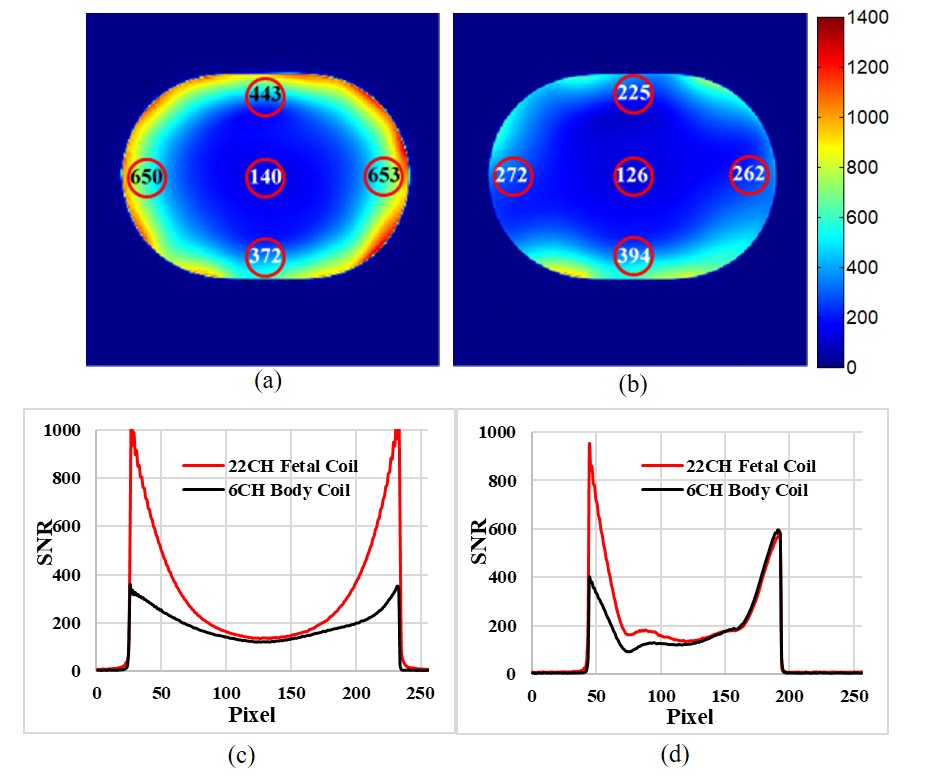
Fig. 3. (a) The SNR map of 22-channel
fetal coil with nine elements of spine coils (a) and 6-channel Siemens body
coil with nine elements of the spine coil array (b) in transverse plane. The SNR variation along the left-right (c) and
up-down (d) direction with different distances away from boundary for proposed
22-channel fetal coil and 6-channel Siemens coil.
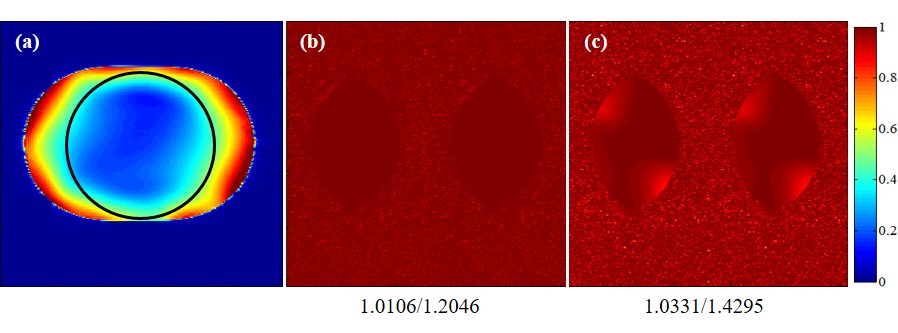
Fig. 4. The location of ROI
in phantom (a). The 1/g-factor of 22-channel fetal coil with nine elements of the
spine coil array (b) and the 6-channel body coil with nine elements
of the spine coil array (c) for reduction factor R = 2.
The numbers
below each map indicate the mean g-factor and the maximum g-factor,
respectively.
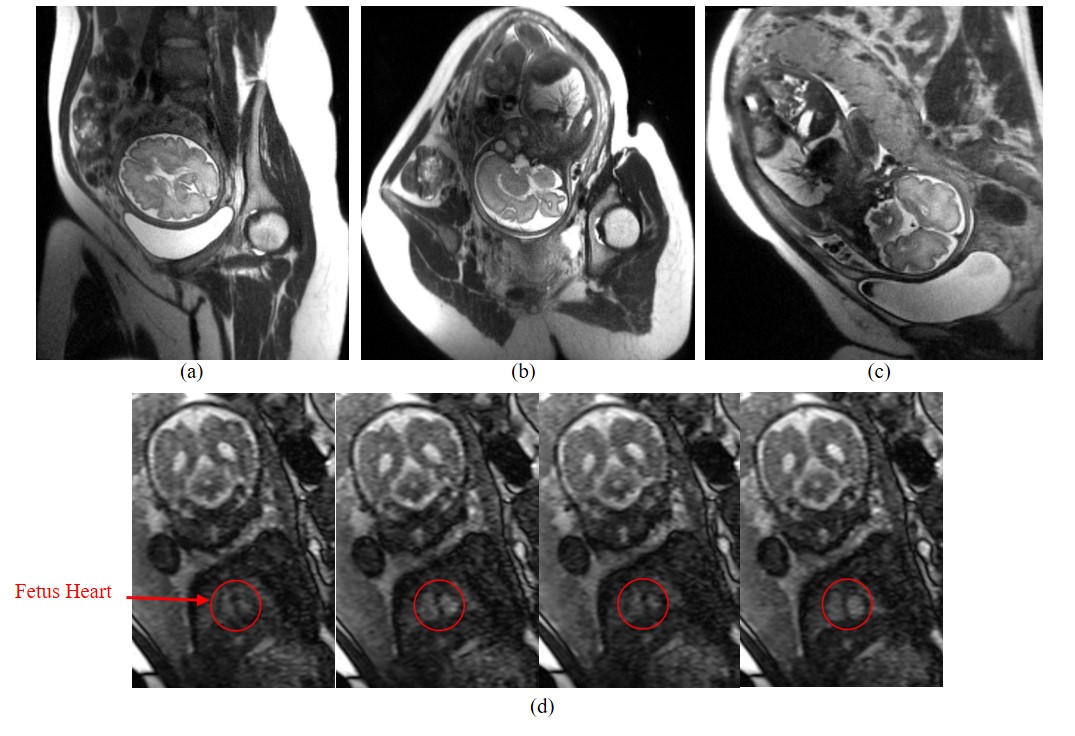
Fig. 5. The fetal head images
of the proposed 22-channel coil with nine elements of a spine coil array in the
transverse (a), sagittal (b) and coronal (c) planes. The multi-slice fetal heart
images acquired by using the proposed 22-channel coil with nine elements of the
spine coil array (d), demonstrating the possibility of fetal cardiac imaging at
3T. The images were shown with the same window level.