1677
Diagnostic value of diffusion tensor imaging and positron emission tomography in early stages of frontotemporal dementia1Department of Neurology, Westfälische Wilhelms University, Münster, Germany, 2Department of geriatric medicine and early rehabilitation, Marien Hospital Herne, Herne, Germany, 3Department of Nuclear Medicine, Westfälische Wilhelms University, Münster, Germany
Synopsis
The study intended to investigate the sensitivity of DTI and FDG-PET in 30 patients with early behavioral variant frontotemporal dementia (bvFTD) despite inconspicuous conventional MRI. Based on individual FDG-PET data analysis, 20 patients were rated as bvFTD “typical” with bifrontal/ bitemporal hypometabolism (bvFTD/PET+) and 10 patients as “not typical/normal” (bvFTD/PET-). DTI voxel-based group analyses revealed bifrontal/ bitemporal microstructural degeneration in all patients. However, individual DTI data analysis revealed alterations in only 14%. Neuropsychological symptoms were associated to DTI and FDG-PET identifiable cerebral changes. Summarising improvement of individual DTI analysis tools is necessary to make this technique applicable for clinical routine.
Introduction
Although the revised diagnostic criteria for behavioral variant frontotemporal dementia (bvFTD)1 allow a more accurate and earlier detection of bvFTD, the diagnosis still remains challenging. The reason for this lies in the suboptimal sensitivity and specifity of structural and molecular neuroimaging tools which are required for diagnosis of bvFTD. Even if advanced MRI techniques such as diffusion tensor imaging (DTI) appeared promising, no studies directly examined and compared the sensitivity of DTI analysis and fluorodeoxyglucose positron emission tomography (FDG-PET) in bvFTD patients. The aim of the study was to investigate the diagnostic value of DTI in comparison to FDG-PET to detect cerebral alterations in early stages of bvFTD despite inconspicuous conventional MRI.Methods
A total of 30 patients with early stages of bvFTD underwent a detailed neurological and neuropsychological examination, a lumbar puncture, cerebral 3T MRI with DTI, and FDG-PET. Based on the individual FDG-PET data analysis, the investigators rated 20 patients as “typical” for bvFTD with bifrontal and/or temporal hypometabolism (bvFTD/PET+; 6 women, 14 men; mean age 64 years) and 10 patients as “not typical” (bvFTD/PET-; 3 women, 7 men; mean age 63 years). DTI data were compared with 42 healthy controls (14 women, 28 men; mean age 60 years) in an individual, voxel-based, and group analysis. To examine the clinical relevance of the findings, associations between pathologically alterated voxels of DTI or FDG-PET results and behavioral symptoms assessed by the Frontal Behavioural Inventory (FBI)1 were estimated by linear regression analyses.Results
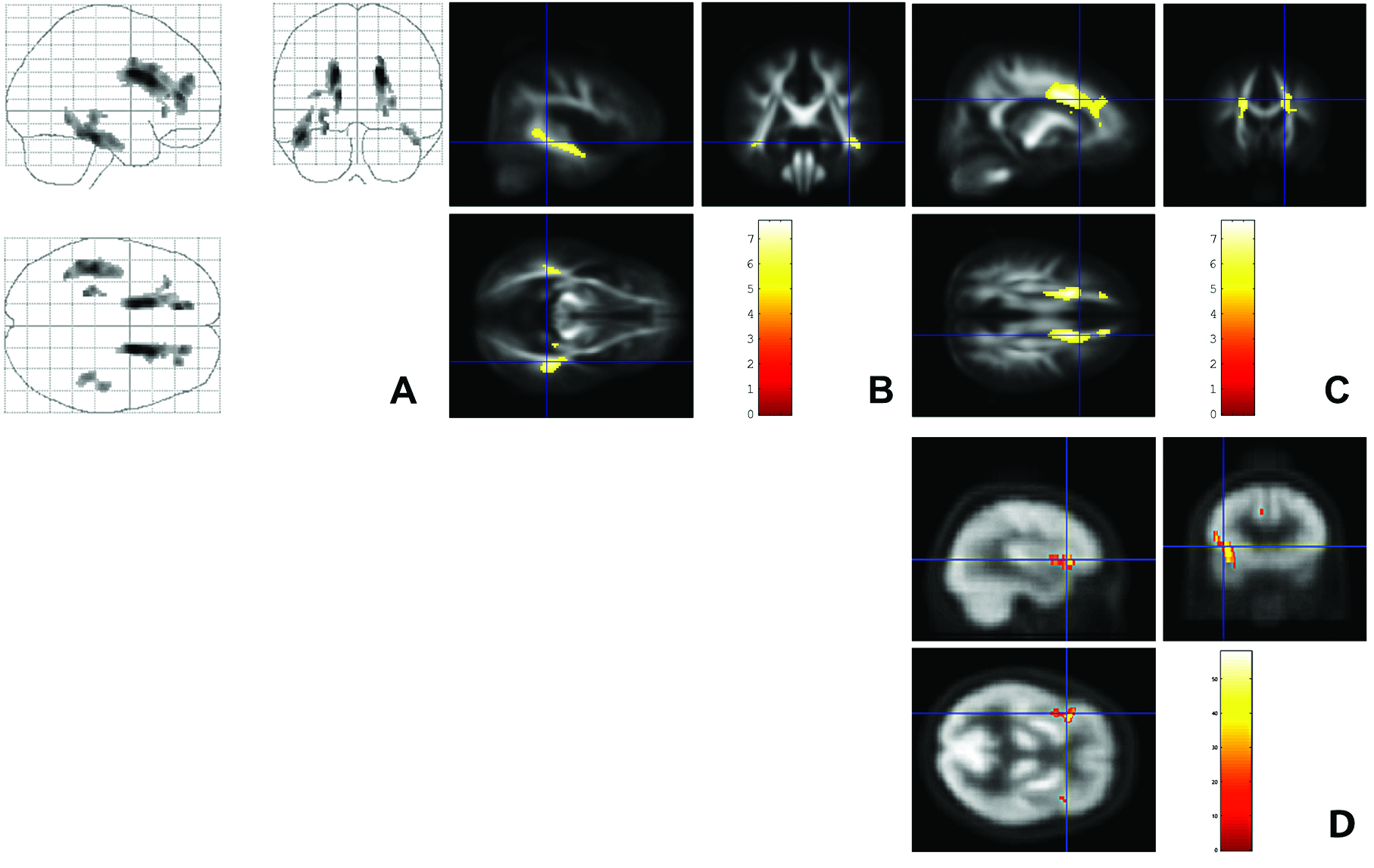
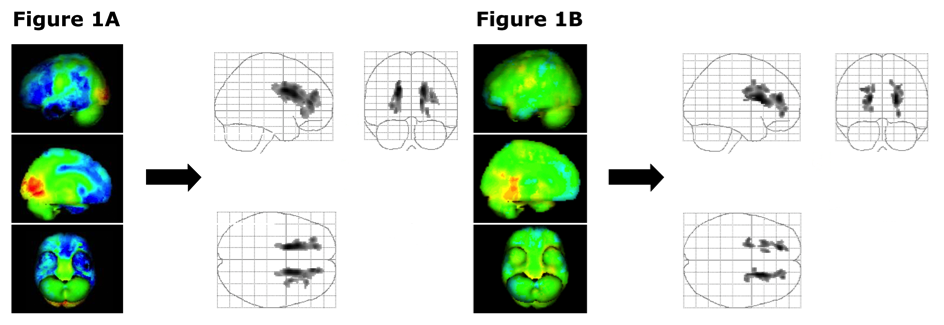
DTI voxel-based and group analyses revealed similar clusters of microstructural degeneration in bifrontal and bitemporal areas in bvFTD/PET+ and bvFTD/PET- groups (Figure 1 and 2). However, when comparing the sensitivity of individual DTI data analysis with FDG-PET, DTI appeared to be less sensitive. In constrast to FDG-PET, which revealed a typical bifrontal and temporal hypometabolism in 66.7% of all patients, DTI revealed bifrontal and bitemporal microstructural alterations in only 14%. Linear regression analyses demonstrated significant correlations of bvFTD typical behavioral symptoms rated by the FBI score with voxels of decreased FA in bifrontal and bitemporal areas (Figure 3 A-C) and with voxels of decreased metabolism of FDG-PET data in bitemporal areas in the whole group of patients (Figure 3 D). After 12 months of follow-up, all patiens finally fulfilled the current diagnostic criteria for "probable" bvFTD due to frontal and/or anterior temporal atrophy in the follow-up MRI1.Discussion
By examing a cohort of patients with early stages of bvFTD but lacking distinctive frontal and/or temporal atrophy on conventional MRI, we could demonstrate that DTI is able to detect functionally relevant neurodegenerative alterations in early stages of bvFTD despite inconspicuous conventional MRI. Although voxel-based and group DTI analyses demonstrated significant microstructural degeneration in bifrontal and bitemporal areas in patients of both groups, the sensitivity of DTI at a single subject level was less sensitive than the FDG-PET analysis. One reason could be a more pronounced difference between normal and pathological values in individual FDG-PET data analysis with less variability compared to single subject DTI data analysis. Another reason could be the fact that metabolic changes depicted by FDG-PET precede microstructural abnormalities detected by DTI.Conclusion
DTI seems to be an interesting and promising tool for detection of functionally relevant neurodegenerative alterations in early stages of bvFTD, even in bvFTD/PET- patients. However, at a single subject level it seems to be less sensitive than FDG-PET. Thus, improvement of individual DTI analysis is necessary to make this technique applicable for clinical routine. Further longitudinal studies with more patients are necessary to investigate if DTI can serve as a marker for early disease detection and differential diagnosis, and to verify its reliability, sensitivity, and specifity at a single subject level, in particular in comparison with other forms of dementia.
Acknowledgements
We thank all participating patients for their contribution to the survey. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.References
1. Rascovsky K, Hodges JR, Knopman D, et al. Sensitivity of revised diagnostic criteria for the behavioural variant of frontotemporal dementia. Brain: a journal of neurology 2011;134(9):2456-77.Figures
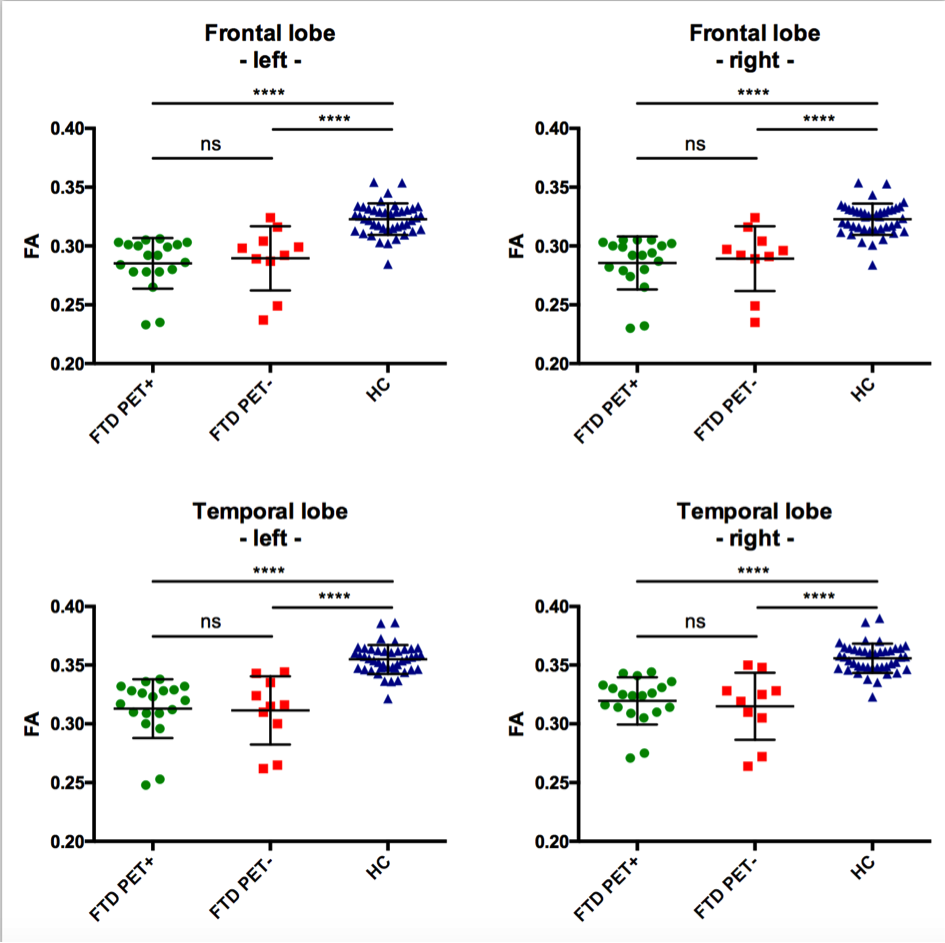
Individual fractional anisotropy of the right and left frontal and temporal lobe of each participant of the group of bvFTD/PET+ and bvFTD/PET- patients and healthy controls. The right and left frontal and temporal fractional anisotropy (FA) values of each patient of both bvFTD/PET+ (FTD PET+) and bvFTD/PET- (FTD PET-) groups were significantly reduced compared to the FA of the group of age- and gender-matched healthy controls (HC) (**** indicate p < 0.0001). There were no significant FA differences between bvFTD/PET+ and bvFTD/PET- patients (n.s. = not significant).