1656
Diffusion MRI as a descriptive imaging marker of the pathogenesis of treatment-resistant depression.1Univ Rennes, INRIA, CNRS, Inserm, IRISA UMR 6074, VISAGES ERL U-1228, F-35000, Rennes, France, 2Academic Psychiatry Department, Centre Hospitalier Guillaume Régnier, Rennes, France, 3EA 4712 Behavior and Basal Ganglia, CHU Rennes, University of Rennes 1, Rennes, France, 4Department of Neuroradiology, University Hospital of Rennes, Rennes, France
Synopsis
Despite the extensive therapy options available for depression, treatment-resistant depression (TRD) occurs in 20-30% of depressed patients. . Consequently, identification of neural changes in TRD could support to better understand the mechanism of resistance and to improve the treatment of individual depressed patients. We aimed to investigate the white-matter microstructure in a sample of depressed patients in which response to treatment was subsequently evaluated 6 months after. Our findings suggest the abnormalities of the white-matter integrity in multiple white matter tracts, such as anterior limb of internal capsule and genu of corpus may play a role in the pathogenesis of treatment-resistant depression.
Introduction
Despite the extensive therapy options available for depression, treatment-resistant depression (TRD) occurs in 20-30% of depressed patients1. Commonly, patients who do not respond present difficulties in social and occupational function, decline of physical health, suicidal thoughts, and increased health care utilization. Consequently, identification of neural changes in TRD could help to understand the mechanism of resistance and to improve the treatment of individual depressed patients.
Structural and functional neuroimaging studies have identified widespread alterations in patients with depression, including abnormalities in fronto-limbic networks. In order to better understand brain correlates of treatment resistance and predict evolution of depressive disorder, there is a growing interest in studying structural abnormalities in TRD. To date, only few magnetic resonance studies have examined the brain structure in TRD2-4. Functional abnormalities were reported within the left amygdala to anterior cingulate when comparing TRD to remitted depression5. Reduced FA values were also found in the ventromedial prefrontal cortex of patients with TRD compared with those with non-TRD2. Thus, multiple brain abnormalities may play a role in the pathophysiology of TRD, notably in limbic regions. In this study, we aimed to investigate the whole-brain white-matter microstructure in a sample of depressed patients in which response to treatment was subsequently evaluated at 6 months.
Material and Methods
LONGIDEP is a routine care cohort of patients suffering from mood depressive disorder who underwent a clinical evaluation, neuropsychological testing and brain MRI. The population sample consists of 57 patients suffering from depression. The Clinical Global Impressions (CGI) improvement Scale was measured to quantify and track patient progress and treatment response after 6 months6. The CGI global improvement measure (CGI-I) is rated from 1 (very much improved) to 7 (very much worse). A composite measure of medication load for each patient was assessed using a previously established method7.
T1-weighted and diffusion tensor imaging (DTI) were acquired on a 3T Siemens Verio scanner with a 32-channel head coil. The diffusion scans were obtained in 30 directions using an EPI sequence with a b-value of 1000s/mm2. The DTI data were processed with the open source medical image processing toolbox Anima8. All the diffusion images underwent (1) eddy current distortion correction, (2) blockwise non-local means filtering and (3) skull stripping followed by (4) a voxel-wise calculation of fractional anisotropy (FA). The resulting maps were normalized into MNI template space. A linear regression analysis was used to assess the correlations between the FA values and the CGI scores (P < 0.05, FDR corrected) by using as covariates age, gender, duration of disease and medication load.
Results
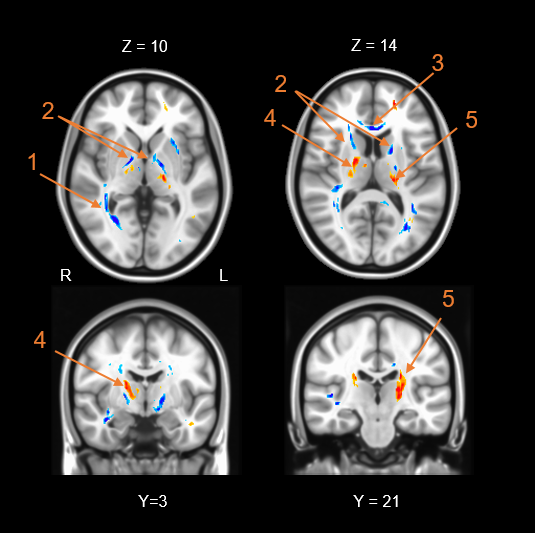
Correlation results of the FA with CGI measures are shown in Figure 1. Linear regression analyses showed negative correlation between the FA values and CGI scores in the right posterior thalamic radiation/superior longitudinal fasciculus (SLF), the bilateral anterior limb of internal capsule (ALIC), the genu of the corpus callosum and the bilateral posterior limb of the internal capsule (PLIC). As shown in figure 1, there were only one brain white matter tract (the posterior limb of the internal capsule) with positive correlation with improvement measure after 6 months.Discussion
The major finding of the present study is that MDD patients showed significant correlation between FA values and treatment-resistant scores in multiple white matter tracts, such as ALIC and genu of corpus. The CGI scores were negatively correlated with FA values in the frontal-subcortical neural circuits, which indicates that the resistant patients have lower FA values than the non-resistant ones. Moreover, previous studies have primarily reported significant white matter reduction in patients with treatment-resistant depression when compared to control subjects in ALIC and corpus callosum2. These tracts connect to the regions related to emotional regulation. This suggest that the degree of white matter disruption in these regions could influence the resistance severity. We also observed that the FA values in the posterior thalamic radiations are associated with treatment resistance. Recently, evidence of an association between this thalamo-cortical fiber tract and treatment-resistant depression has been reported 9. Indeed, recent resting-state functional MRI study reported significantly disrupted connectivity between the thalamus and several brain regions in patients with TRD10. This analysis also revealed increased FA in the bilateral posterior limbs of the internal capsule in patients with treatment-resistant depression. In summary, our findings suggest that the abnormalities of the white matter integrity of neuronal tracts connecting cortical and subcortical nuclei, thalamus with the cerebral cortex and two cerebral hemispheres may play a role in the pathogenesis of treatment-resistant depression.Acknowledgements
Julie Coloigner was supported by a INCR fellowship.
MRI data acquisition was supported by the Neurinfo MRI research facility from the University of Rennes I. Neurinfo is granted by the the European Union (FEDER), the French State, the Brittany Council, Rennes Metropole, Inria, Inserm and the University Hospital of Rennes.
References
1. Greden, J. F. (2001). The burden of disease for treatment-resistant depression. Journal of Clinical Psychiatry, 62 (Suppl 16), 26–31.
2. Guo, W. B., Liu, F., Chen, J. D., Xu, X. J., Wu, R. R., Ma, C. Q., ... & Chen, H. F. (2012). Altered white matter integrity of forebrain in treatment-resistant depression: a diffusion tensor imaging study with tract-based spatial statistics. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 38(2), 201-206.
3. de Diego-Adelino, J., Pires, P., Gomez-Anson, B., Serra-Blasco, M., Vives-Gilabert, Y., Puigdemont, D., ... & Portella, M. J. (2014). Microstructural white-matter abnormalities associated with treatment resistance, severity and duration of illness in major depression. Psychological medicine, 44(6), 1171-1182.
4. Sandu, A. L., Artiges, E., Galinowski, A., Gallarda, T., Bellivier, F., Lemaitre, H., ... & Paillère Martinot, M. L. (2017). Amygdala and regional volumes in treatment‐resistant versus nontreatment‐resistant depression patients. Depression and Anxiety.
5. Lui, S., Wu, Q., Qiu, L., Yang, X., Kuang, W., Chan, R. C., ... & Gong, Q. (2011). Resting-state functional connectivity in treatment-resistant depression. American Journal of Psychiatry, 168(6), 642-648.
6. Busner, J., & Targum, S. D. (2007). The clinical global impressions scale: applying a research tool in clinical practice. Psychiatry (Edgmont), 4(7), 28
7. Sackeim, H. A. (2001). Functional brain circuits in major depression and remission. Archives of General Psychiatry, 58(7), 649-650.
8. ANIMA: open-source software for medical image processing, https://github.com/Inria-Visages/Anima-Public/wiki.
9. Duffy, S. L., Paradise, M., Hickie, I. B., Lewis, S. J., Naismith, S. L., & Lagopoulos, J. (2014). Cognitive impairment with and without depression history: an analysis of white matter microstructure. Journal of psychiatry & neuroscience: JPN, 39(2), 135.
10. Yamamura, T., Okamoto, Y., Okada, G., Takaishi, Y., Takamura, M., Mantani, A., ... & Yamawaki, S. (2016). Association of thalamic hyperactivity with treatment-resistant depression and poor response in early treatment for major depression: a resting-state fMRI study using fractional amplitude of low-frequency fluctuations. Translational psychiatry, 6(3), e754.
Figures