1536
Functional MRI at ultra-high field strength (11.7 T) for evaluation of rectal cancer stromal heterogeneity ex vivo: correlation with histopathology1Radiation Oncology, Liverpool Cancer Therapy Centre, Liverpool Hospital, Sydney, Australia, 2Sydney West Radiation Oncology Network, Westmead, Blacktown and Nepean Hospitals, Sydney, Australia, 3Faculty of Medicine, University of New South Wales, Sydney, Australia, 4Ingham Institute for Applied Medical Research, Sydney, Australia, 5School of Medicine, Western Sydney University, Sydney, Australia, 6Nanoscale Organisation and Dynamics Group, Western Sydney University and National Imaging Facility, Sydney, Australia, 7Anatomical Pathology, Liverpool Hospital, Sydney, Australia
Synopsis
Diffusion Tensor Imaging (DTI) MRI at ultra-high field (11.7 T) was used to examine the stromal ultrastructure of malignant and normal rectal tissue ex vivo, and findings were correlated with histopathology. DTI was able to distinguish tumour from desmoplasia: tumour was found to have isotropic diffusion, whereas desmoplastic reaction or fibrous tissue had moderately anisotropic diffusion. DTI was useful in assessing depth of tumour infiltration into rectal wall: tumour was able to be distinguished from muscularis propria which was highly organised and anisotropic. This study showed that DTI-MRI can assist in more accurately defining tumour extent in rectal cancer.
Introduction
Tumour stroma evolves during cancer progression, and is associated with increased extracellular matrix. The increased deposition of extracellular matrix in tumours is known as desmoplasia, and characteristic of many advanced cancers.1,2 Current clinical MRI techniques in rectal cancer have limited ability to examine cancer stroma. The differentiation of tumour from desmoplasia or fibrous tissue remains a challenge. MRI is unable to differentiate Stage T1 from T2 (invasion of muscularis propria) tumours.3 Diffusion tensor imaging (DTI) MRI can probe tissue structure and organization (anisotropy). To our knowledge, there have been no DTI-MRI studies assessing rectal cancer ex vivo. The purpose of this study was to examine DTI-MRI derived biomarkers of rectal cancer stromal heterogeneity at ultra-high field (11.7 T) ex vivo, and correlate with histopathology.Methods
Ten rectal tissue specimens were collected from 5 patients with a diagnosis of rectal cancer undergoing surgery through the Ingham Institute Cancer Biobank. Tissue specimens were fixed in 10% formalin and embedded in 1% agarose containing 2mM gadopentetate dimeglumine for MR imaging. Tissue samples were scanned on the Bruker Avance II 500 MHz (11.7 T) wide bore MRI Spectrometer at Western Sydney University Biomedical Magnetic Resonance Facility. An MRI FLASH sequence with 100 µm voxels was acquired to facilitate anatomical registration of MRI with histopathology. DTI-MRI was acquired with isotropic 200 µm voxels with b-values 200, 800 and 3200 s/mm2. The echo time was 26 ms, repetition time was 900 ms, diffusion gradient separation was 15 ms, and diffusion gradient duration was 5 ms. Eight diffusion directions were acquired with 3 diffusion experiments per direction. An A0 image was acquired. Colour-encoded DTI maps were generated. Fractional Anisotropy (FA) values were calculated using the formula,
$$FA=√(3/2) (√((λ1-⟨λ⟩)^2+(λ2-⟨λ⟩)^2+(λ3-⟨λ⟩)^2 ) )/√((〖λ1〗^2+ 〖λ2〗^2+ 〖λ3〗^2))$$
where the λ1, λ2, λ3 and (λ) are the diffusion eigenvalues in three orthogonal directions and their average value, respectively. FA maps were generated with FA = 0 indicating isotropic diffusion (no organisation) and FA = 1 indicating anisotropic diffusion. Specimens were examined by light microscopy using H&E and Masson Trichome stains. Regions of interest for analysis were annotated on digital histopathology by a Gastrointestinal Pathologist, for correlation with DTI-MRI.
Results
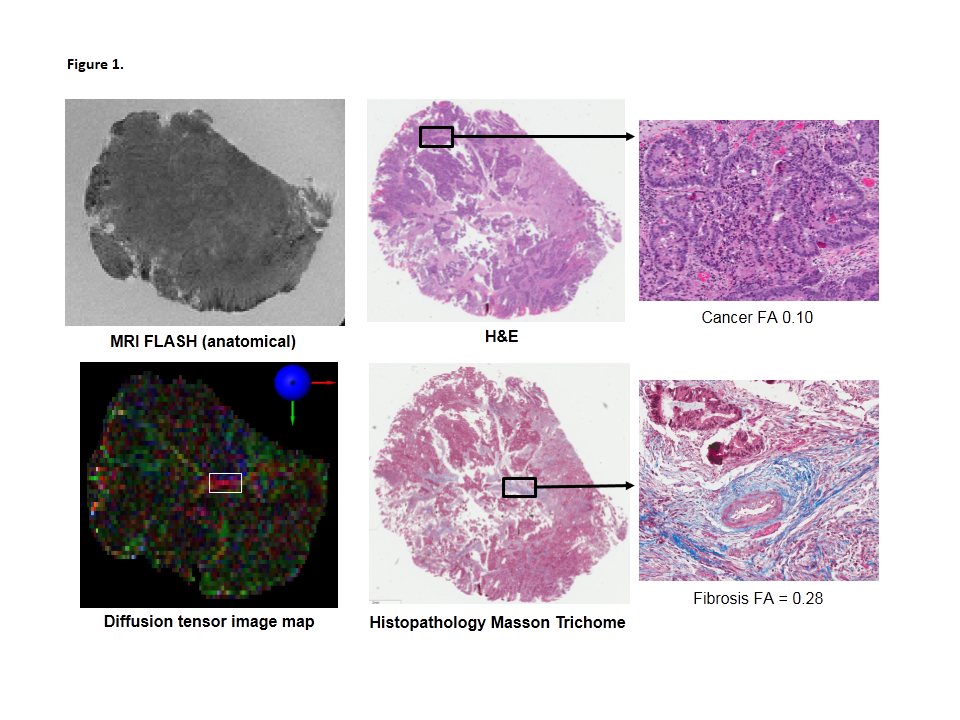
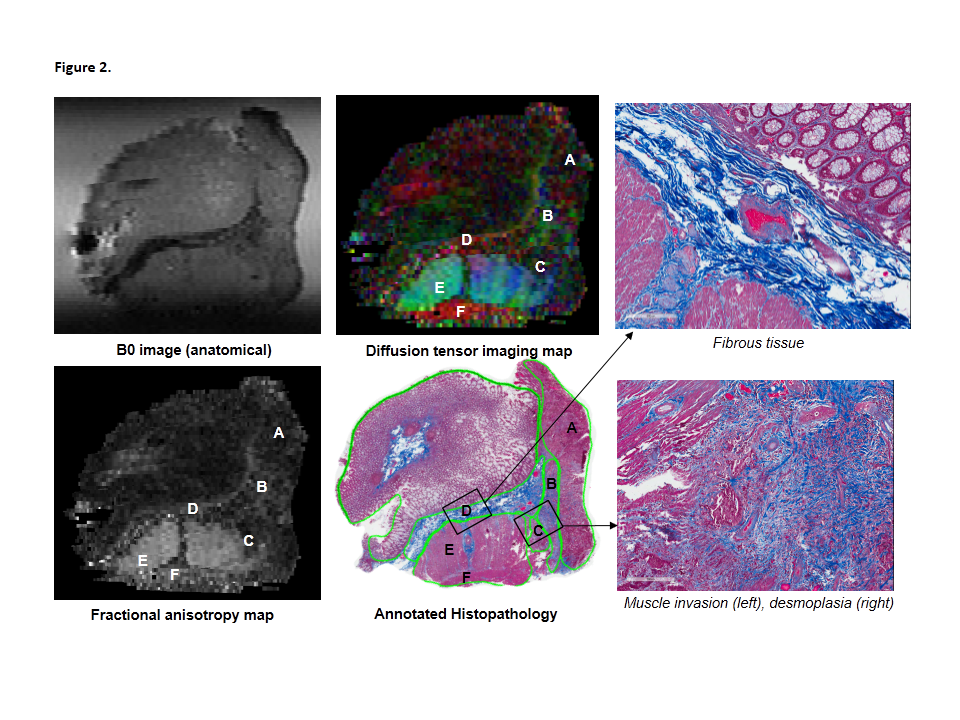
Ultra-high resolution DTI-MRI was able to depict stromal heterogeneity in rectal cancer. Examination of rectal cancer specimen DTI and FA maps, and histopathology demonstrated low FA in tumour regions, indicating a lack of stromal organisation and isotropic diffusion in tumour (FA 0.14 – 0.16). DTI-MRI was able to visualise heterogeneity within cancer stroma, with regions of moderate FA corresponding to desmoplasia (FA 0.25 – 0.40) or normal fibrous tissue (FA 0.28 – 0.41) (Figures 1 and 2). Cancer invasion into muscularis propria (Stage T2) was able to be identified on DTI (Figure 2). Muscularis propria was clearly distinguished from tumour, with muscularis propria appearing highly anisotropic on DTI and FA maps (FA 0.65).
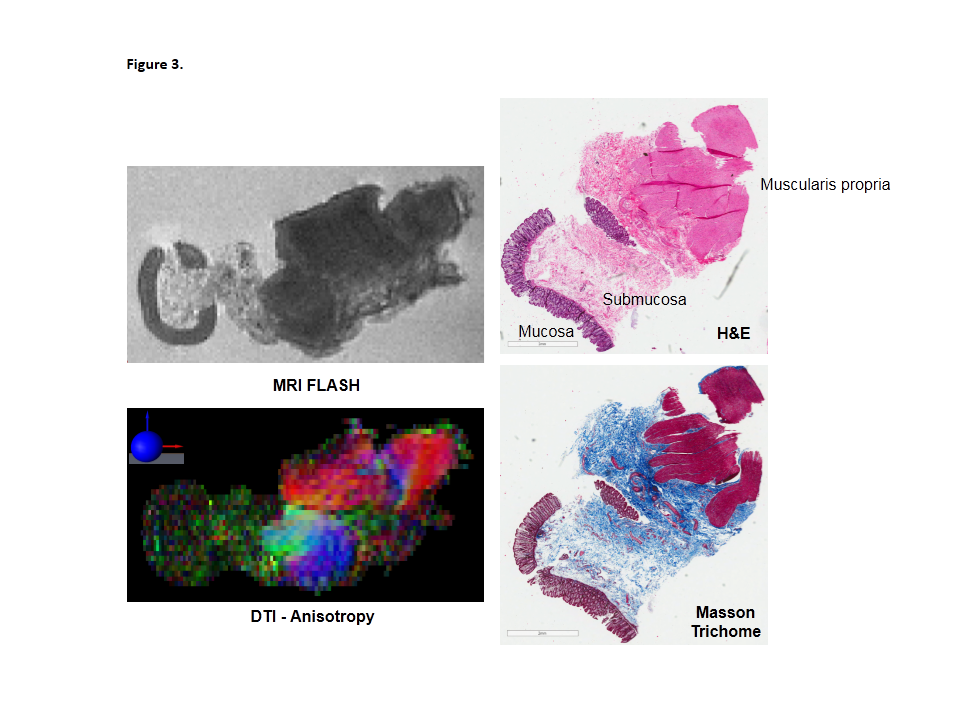
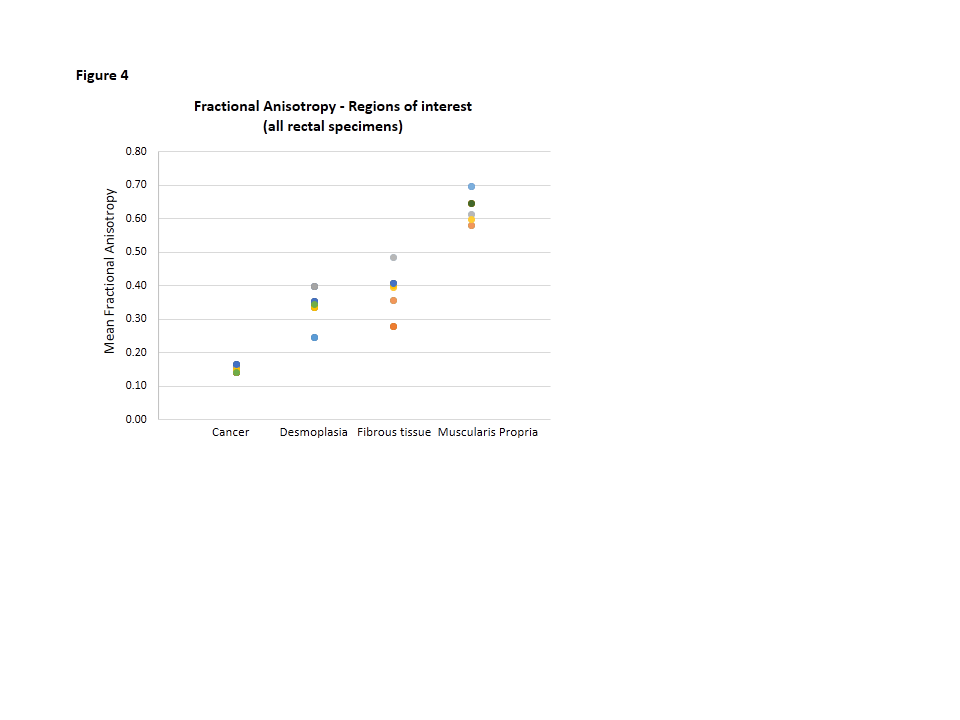
On the DTI and FA maps of adjacent normal rectal specimens, muscularis propria was clearly anisotropic (FA 0.58 – 0.70) (Figure 3). The different muscular fibre orientations of the inner circular, and outer longitudinal layers were clearly visible on the colour-coded DTI maps. The mean FA of regions of interest for all rectal specimens are shown in Figure 4.
Discussion
This MRI-histopathology correlative study demonstrated the ability of DTI-MRI to assess rectal cancer stromal heterogeneity. A desmoplastic reaction in rectal cancer can pose challenges in accurate staging of rectal cancer, as desmoplastic stranding can appear similar to tumour on MRI resulting in overestimation of tumour extent. DTI showed that tumour lacks organisation and consequently has relatively isotropic diffusion (low FA), in contrast desmoplasia and normal fibrous tissue have moderate stromal organisation and anisotropy. Normal muscularis propria had a highly organised appearance and anisotropic diffusion. DTI was able to visualise tumour infiltration and disruption of the muscularis propria at the invasive cancer front. This study has shown that FA constitutes a novel MRI biomarker of rectal cancer stromal organisation and infiltration. DTI-MRI may add value to conventional MRI in more accurately defining extent of tumour invasion, which may assist with treatment planning.Conclusion
This exploratory study demonstrated DTI-MRI is able to differentiate tumour from desmoplasia and fibrous tissue ex vivo. DTI was also able to identify cancer invasion into muscularis propria. Thus, DTI-MRI can provide clear characterisation of tumour stromal heterogeneity and accurate delineation of tumour extent in rectal cancer, and warrants further investigation.Acknowledgements
No acknowledgement found.References
1Hanahan et al. Cell. 2011:144:646
2Kalluri et al. Nat Rev Cancer 2006:6:392
3Beets-Tan et al Eur Radiol 2013:23:2522
Figures