1503
Feasibility Study for Off-Center Targets using ExAblate transcranial MR Guided Focused Ultrasound (tMRgFUS) System1Department of Diagnostic Radiology and Nuclear Medicine, University of Maryland Medical Center, Baltimore, MD, United States
Synopsis
Recent approval by the FDA for treating essential tremors has created increased interest in targeting other critical regions within the brain. Relatively low frequency 220kHz tMRgFUS system has the potential to reach off-center targets compared to the 670kHz system used for essential tremor treatment. In this work, we assess the feasibility of the 220kHz reaching targets such as the central lateral thalamus (CL) due to its role in neuropathic pain and the more laterally located temporal lope for the role it plays in temporal lobe epilepsy. Results suggest that temporal lobe interventions are possible but may require a careful optimization.
Introduction
tMRgFUS is gaining popularity with the FDA approval of the procedure to treat essential tremors. There is growing interest in treating targets away from the center of the brain and extend its application from neuromodulation to blood-brain barrier opening. However, the heat absorption of skull is proportional to the frequency of ultrasound, and the amount of heat deposited on the skull can be significant decreased in cases where the focal target is far from the center of brain. In this study, the treatment envelope of Insightec 220kHz transcranial MR guided Focused Ultrasound (tMRgFUS) system is investigated and compared with the 670kHz system.Methods
CT head images were obtained on a 64-slice CT scanner (Philips Brilliance 64, Philips, WA) prior to treatment. CT Skull imaging parameters included slice thickness of 1 mm with zero spacing, and 144 reconstructed slices with matrix size 512 x 512, resulting in a voxel size of 0.48 x 0.48 x1 mm. Similarly, T2-weighted MR images were obtained at a TE/TR=80/4000ms covering the entire brain at 3 mm thick slices and targets for intervention were identified on these images. The acoustic properties of skull were derived from image intensity distribution of CT images1 to simulate the acoustic field. A non-linear acoustic model was employed to simulate the acoustic field by solving the full Westervelt equation2 for the1024-element ultrasound transducer array. Temperature simulation was estimated by solving the inhomogeneous Pennes equation of heat conduction3. This model used in this study was previously validated on the clinical results from a previous study4 that targeted the VIM, based on the MR thermometry images. Based on the ration of temperature rise on the skull to that reached at the targeted brain tissue, the treatment envelope of the 220 kHz tMRgFUS was then computed.Results and Discussions
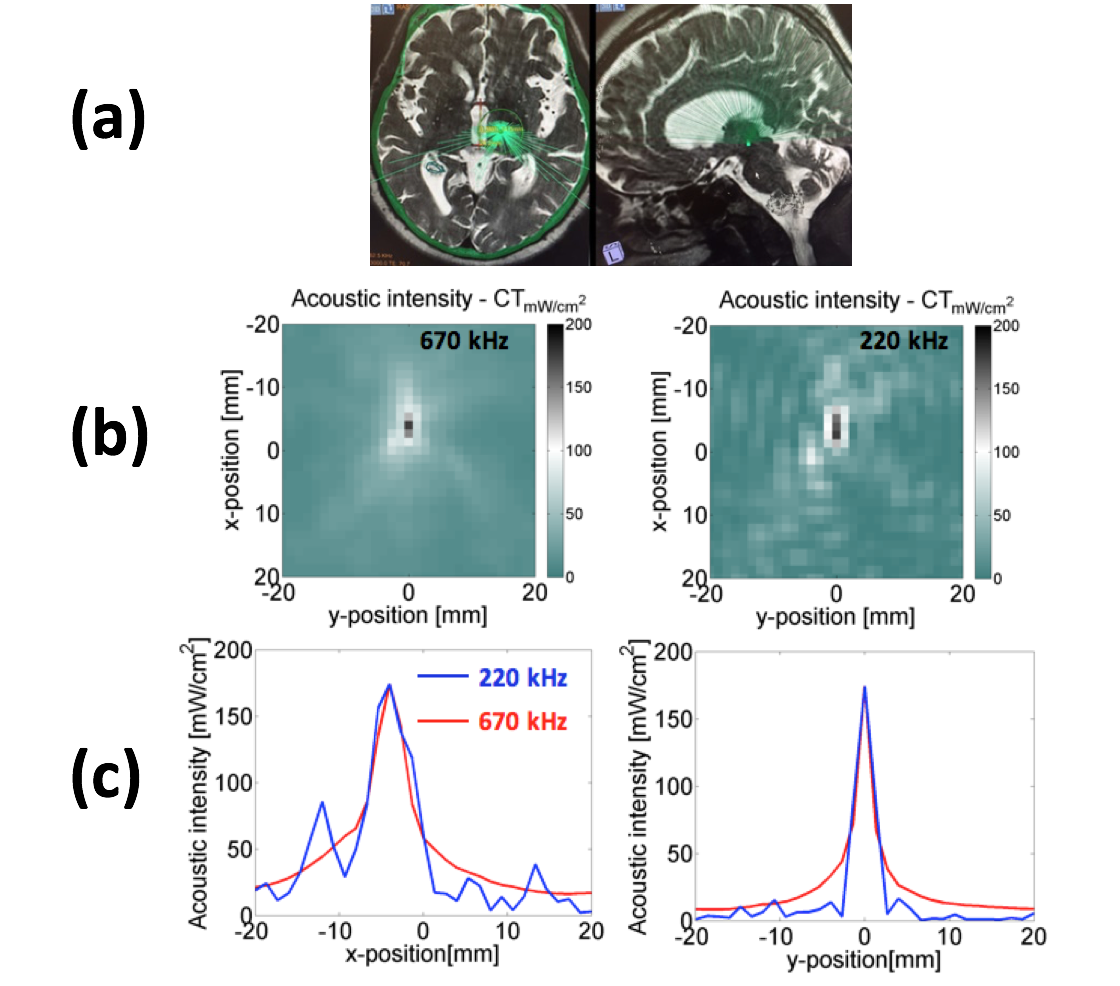
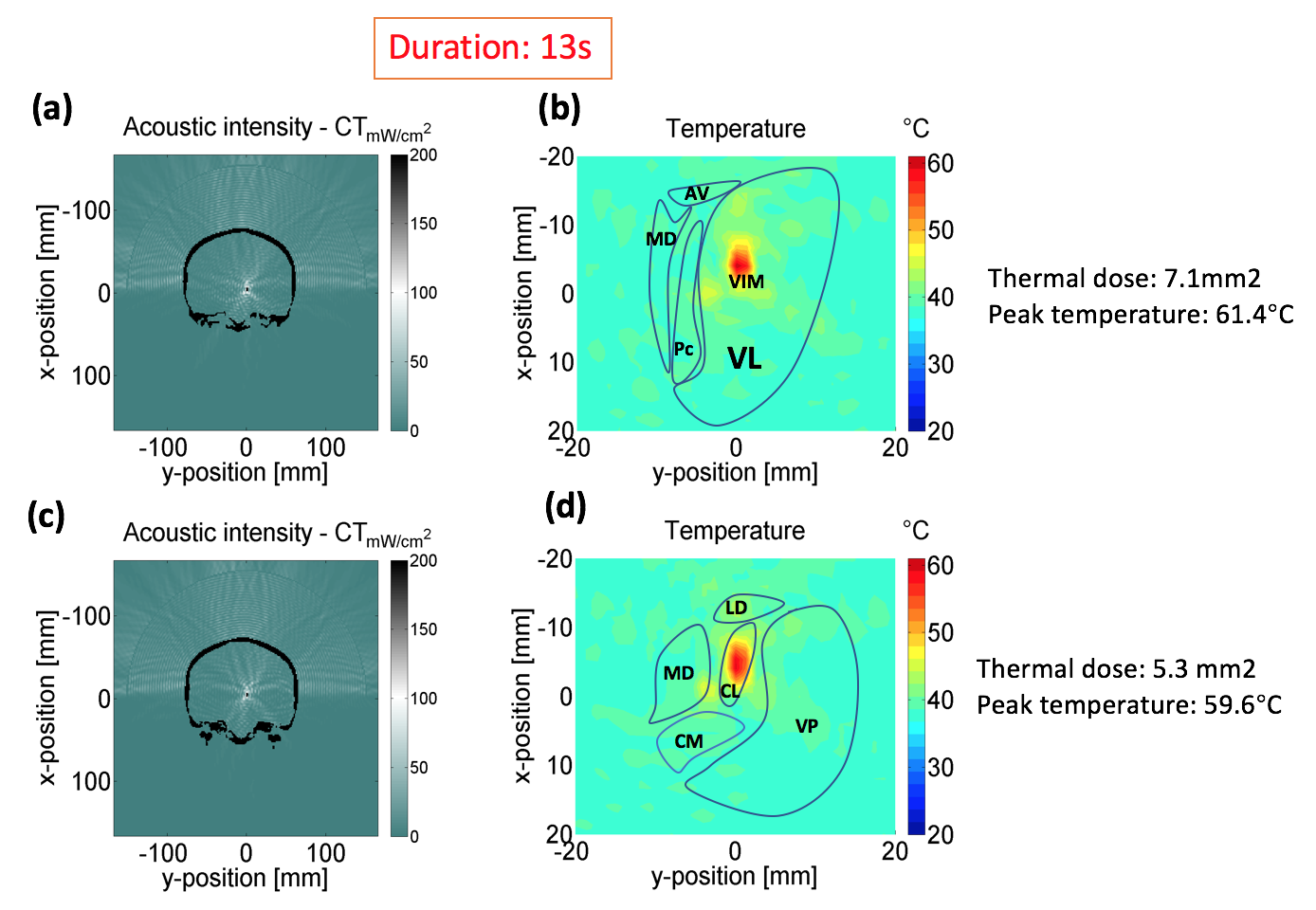
The treatment location of essential tremor at VIM is shown in Fig. 1(a). The simulated acoustic focal zones in coronal view for 670kHz and 220kHz are shown in Fig. 1(b). The focal area of 220kHz is bigger and blunter compared to that of 670kHz. However, it should be noted that for the same temperature rise at the target, 670kHz creates more skull heating than 220kHz due to low absorption of 220kHz at the skull. Fig. 1(c) shows medial-lateral acoustic intensity distribution (left), inferior-posterior acoustic intensity distribution (right) for both frequencies. To obtain an appreciation for temperature rise, we simulated conditions where the sonication duration was maintained for 13s, Fig. 2 shows the simulated acoustic field and temperature field of 220kHz when targeting the VIM is shown in (Fig. 2a and b) with the temperature rise being shown in reference to the Morel atlas in Fig 2b. Simulated acoustic field and temperature field when targeting the CL is shown in Fig. 2(c) and (d). Given that the CL and VIM are not too far from each other it is not surprising that that temperature and thermal maps are similar for these two targets.
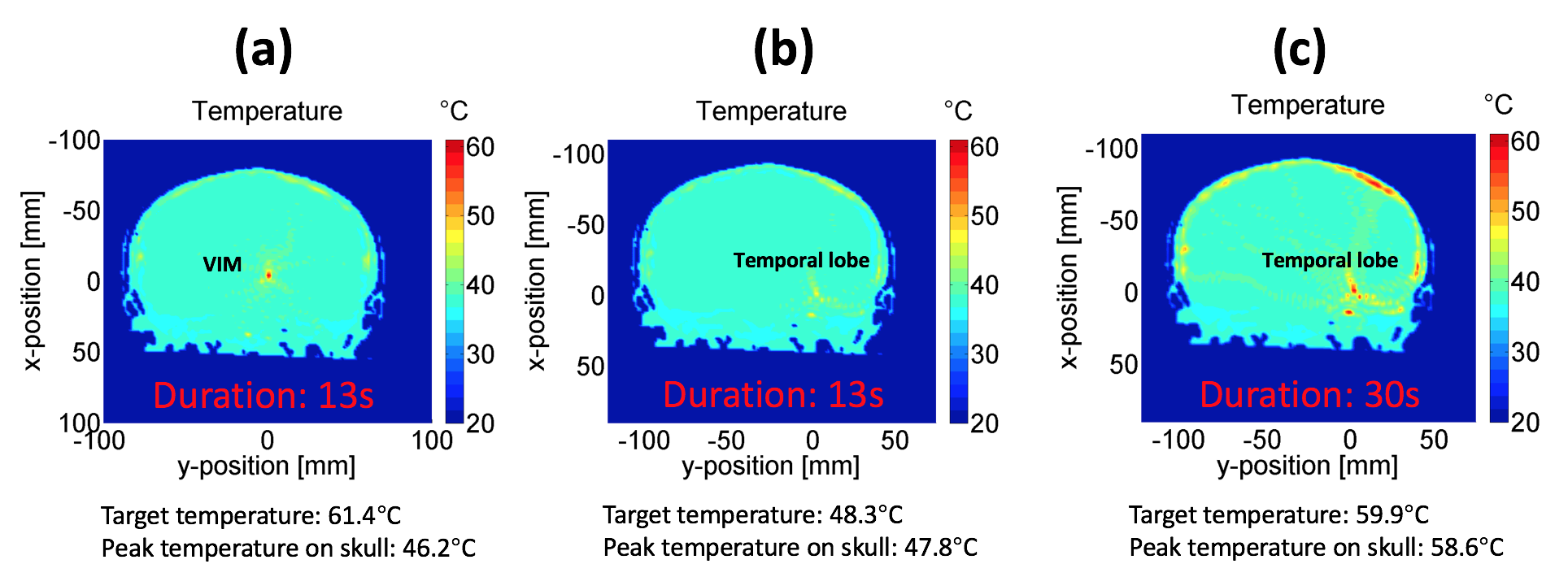
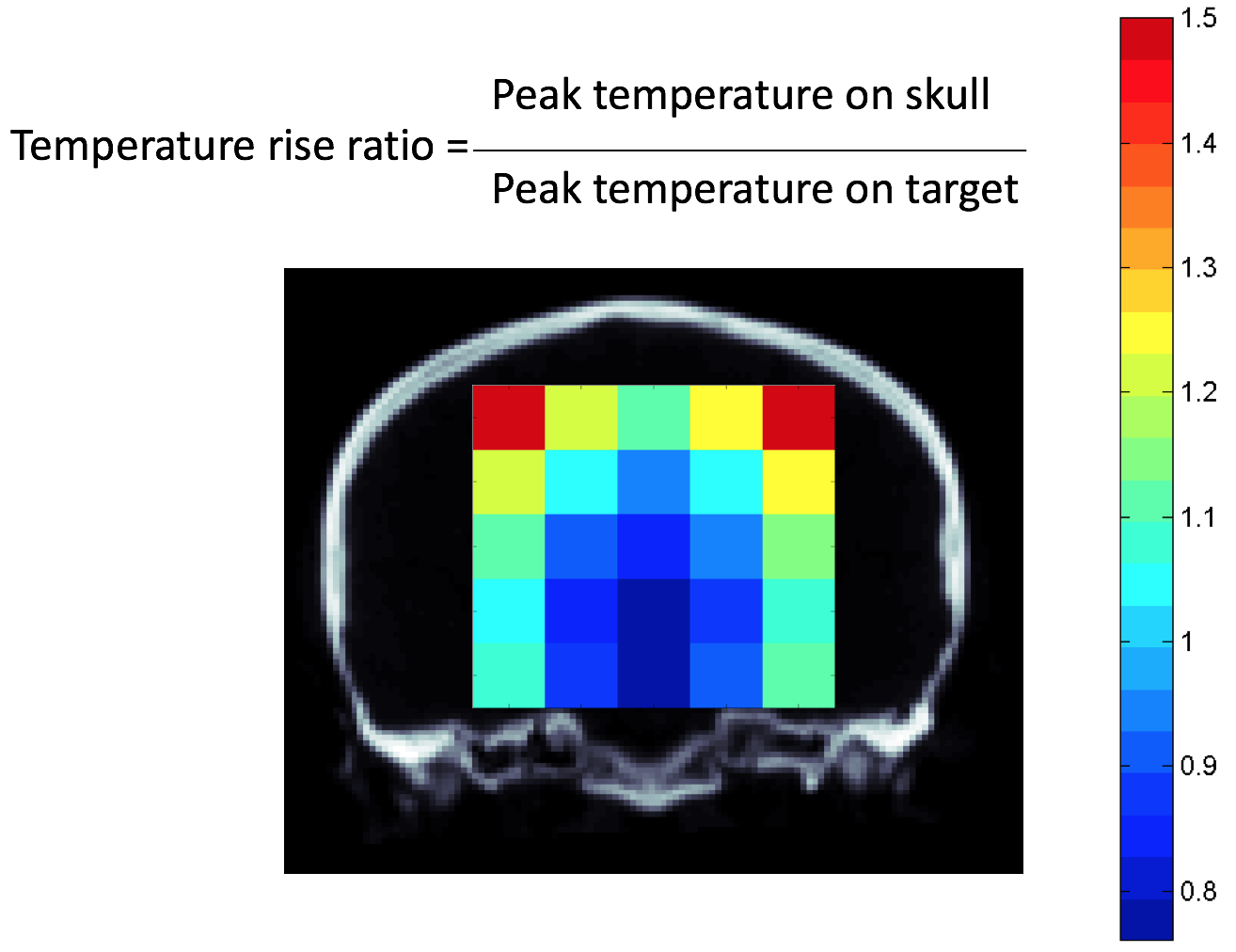
The simulated temperature while targeting the regions of the VIM and the temporal are present in Fig. 3. Fig 3(a) shows simulated temperature field at 13s while the focal target is at VIM. Fig. 3(b) shows simulated temperature field at 13s while the focal target is at temporal lobe with the same power. Fig. 3(c) shows simulated temperature field at 30s while the focal target is at temporal lobe in order to achieve similar maximum temperature rise as VIM. However this maximum temperature at the target generates a significant amount of heat at the skull surface. This suggests that if ablative temperatures are required near to the temporal lobe, then sufficient steps must be taken to dissipate the heat at the skull. The peak temperature simulation results from across different locations of the whole brain as shown in Fig. 4 reveals the possibility for various levels of interventions and is based on peak temperature on the skull over peak temperature on skull over peak temperature attainable at the target.
Conclusions
The study investigated the feasibility of 220kHz tMRgFUS on the treatment at CL (neuropathic pain) and temporal lobe (epilepsy). The heat absorption of skull is lower for 220kHz compared with 670kHz, especially for the cases when the focal target is far from the center of brain. When targeted on CL, heat generation is slightly less efficient than VIM. When targeted on temporal lobe, heat generation rate is significant decreased. A compromise between lower energy, longer exposure duration and efficient heat dissipation at the skull may be required for effective intervention in the case of temporal lobe epilepsy.Acknowledgements
No acknowledgement found.References
1. Aubry J, Tanter M, Gerber J, Thomas L and Fink M. Optimal focusing by spatio-temporal inverse filter: part II. Experiments. J. Acoust. Soc. Am., 2001.
2. M Hamilton, D Blackstock, Nonlinear Acoustics, Academic Press., 1998.
3. Pennes H. Analysis of tissue and arterial temperature in the resting human forearm. J. Appl. Physiol., 1948.
4. Guo S, Zhuo J and Gullapalli R. Water diffusivity changes in the brain following exposure to low levels of focused ultrasound energy. Honolulu, United States: ISMRM; 2017.
Figures