1499
Passive Marker Tracking with Phase-Only Cross Correlation (POCC) in Highly Undersampled Radial Images: Improvements by Point-Spread-Function Considerations1Dept. of Radiology, Medical Physics, Medical Center University of Freiburg, Faculty of Medicine, University of Freiburg, Freiburg, Germany
Synopsis
Passive tracking with the phase-only cross correlation (POCC) algorithm can be used to accurately detect the position of MR-markers for needle procedures. The POCC tracking sequence continuously visualizes the planned needle trajectory during movement, however, image acquisition is interleaved with the measurement of two tracking images which degrades the temporal resolution. Here, it is shown that highly undersampled radial imaging together with the incorporation of the point-spread-function into the POCC algorithm can track the marker at substantially shorter acquisition times. This is an important step to improve the overall temporal resolution and might help to reduce durations of percutaneous procedures.
Introduction
Safe and effective MR-guided interventions require fast and reliable localization of the interventional device. This can be achieved with MR-safe passive markers which have been proposed as needle guides for MR-guided percutaneous biopsies1. It has been shown that detection of these markers can efficiently be performed via a phase-only cross correlation (POCC) algorithm2-4. Here, the marker is localized in 2 tracking images orthogonal to the marker, and the position information extracted via the POCC algorithm is then used to align a targeting image with the marker’s symmetry axis (i.e., the planned needle trajectory). This way, the sequence automatically follows the marker and can be used during targeting. Even with acceleration techniques such as simultaneous multislice (SMS) imaging, acquisition of the tracking images require half of the duration of one tracking cycle (i.e. acquisition of two tracking images and one targeting image)5. As the tracking images do not contain any clinically relevant information, their acquisition times should be as short as possible to provide targeting images at a higher sampling rate. Based on previous work on accelerated tracking via radial undersampling6, it is shown that reliable and accurate marker tracking can be achieved even in highly undersampled radial data by incorporating the point-spread-function (PSF) into the POCC algorithm. The concept is implemented and compared to conventional POCC marker tracking.Methods
The implemented POCC tracking sequence is designed to track a cylindrical needle guide filled with contrast agent (Magnevist®/H2O: 1/200, Bayer Schering Pharma AG, Berlin, Germany). Two orthogonal FLASH tracking images are acquired in which the marker appears as a ring and can automatically be detected via computation of the maximum of the POCC function
$$POCC(x,y) = \frac{I(x,y)}{\|I(x,y)\|}*\frac{M(x,y)}{\|M(x,y)\|}.$$
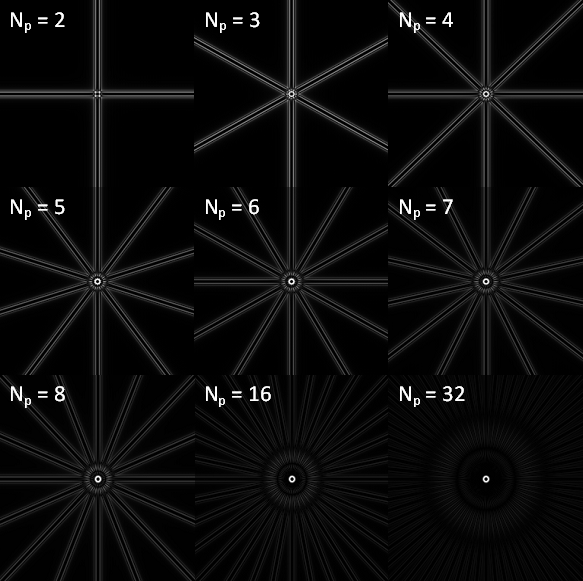
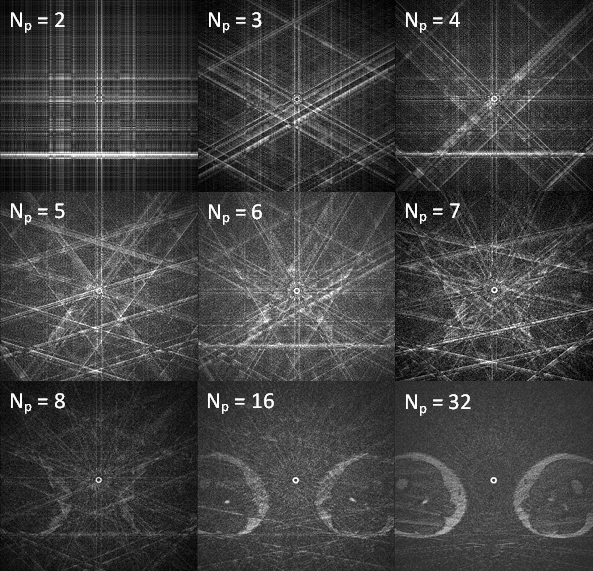
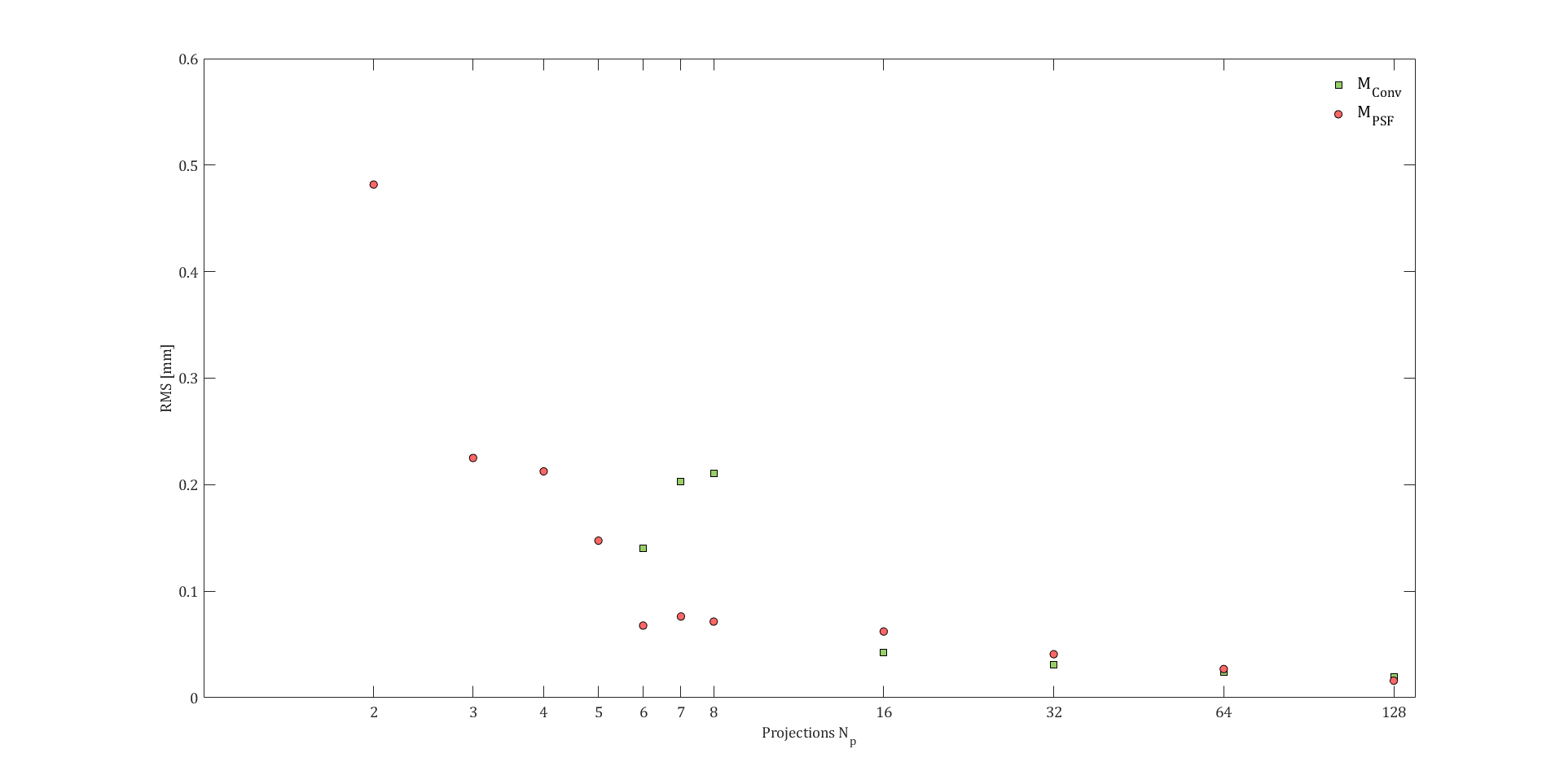
The POCC function calculates the normalized convolution between the acquired image $$$I(x,y)$$$ and a simulated mask image $$$M(x,y)$$$ synthesized from the marker dimensions and the MR sequence parameters (field of view (FOV) and matrix size) efficiently in k-space. The position information is then used to align a targeting image with the marker axis and to visualize the planned needle trajectory to enable online targeting during an interventional procedure. The temporal resolution of the sequence considerably depends on the acquisition time of the tracking images, and even with SMS acceleration, acquisition of the tracking images takes half the time of one tracking cycle5. To realize substantially faster marker tracking, a radially undersampled imaging in combination with a modified POCC detection algorithm is implemented. Therefore, the synthetic mask image ($$$M_\text{PSF}$$$; cf. Fig.1) is calculated which also incorporates the PSF for the radial undersampling scheme7. To assess if the projection specific masks yield improved marker tracking in comparison to the conventional POCC tracking, the marker was placed between the thighs of a volunteer and images of the marker cross section were acquired in a 1.5T whole body MR system (MAGNETOM Symphony, Siemens Healthcare, Erlangen, Germany) using the body array and the spine coil for reception. Images were collected with different numbers of evenly spaced projections ($$$N_p=256,~128,~64,~32,~16,~8,~7,~6,~5,~4,~3,~2)$$$, and for each projection number, 50 images were obtained (TR/TE=6/3ms, α=30°, FOV: 300×300mm, matrix: 256×256). Online image reconstruction was done using Kaiser-Bessel regridding and subsequent Fourier-Transformation. Afterwards, POCC detection was carried out for each image with subpixel precision2 using the conventional mask images $$$M_\text{Conv}$$$ and the corresponding modified masks $$$M_\text{PSF}$$$. For each data set, the root-mean-square error $$$RMS=\sqrt{s_{x}^2+s_{y}^2}$$$ was calculated from the standard deviations $$$s_x$$$ and $$$s_y$$$ of the positions from the POCC maximum, if the detection was successful in over 90% of the images (Fig. 3). The marker was deemed “not detected”, if the determined position was outside the inner marker radius (compared to the image with 256 projections).
Results & Discussion
Using a conventional mask image for POCC detection of the ring, tracking of the marker cross section was possible for $$$N_p≥6$$$ while maintaining the detection accuracy. Lower $$$N_p$$$ leads to failure of detection in over 10% of all images, which is unsuitable for clinical work. POCC detection with projection-specific masks was possible in all images even for $$$N_p=2$$$ at a reasonable tracking accuracy (Fig 3). In this case, the deviation leads to a targeting accuracy of 1.7±0.2mm which is an acceptable accuracy for a clinical setting4. Our results show that passive marker detection can be achieved with as low as two radial projections if the specific PSF is considered in the computation of the mask used in the POCC algorithm. For a TR of 6ms, the acquisition of the tracking images and computation of the marker position was completed within 24ms. With incorporation of this technique into the tracking sequence the marker tracking would take a negligible time and would allow targeting of moving structures.Acknowledgements
We would like to thank for the grant support from the DFG under grant number HA 7006/1-1.References
1. Beyersdorff, D. et al. MR Imaging–guided Prostate Biopsy with a Closed MR Unit at 1.5 T: Initial Results1. Radiology 234, 576–581 (2005)
2. de Oliveira A, et al. Automatic passive tracking of an endorectal prostate biopsy device using phase-only cross-correlation. Magn Reson Med 59:1043–1050 (2008)
3. Krafft AJ, et al. Passive marker tracking via phase-only cross correlation (POCC) for MR-guided needle interventions: Initial in vivo experience. Physica Medica 29:607-614 (2013)
4. Zamecnik P, et al. Automated Real-time Needle-Guide Tracking for Fast 3-T MR-guided Transrectal Prostate Biopsy: A Feasibility Study. Radiology 273:879-886 (2014)
5. Reichert A, et al. Simultaneous slice excitation for accelerated passive marker tracking via phase-only cross correlation (POCC) in MR-guided needle interventions. Proc. Intl. Soc. Mag. Reson. Med. 25 (2017)
6. Reichert A, et al. Investigation of Phase-only Cross Correlation (POCC) for Passive Marker Tracking with a limited Number of Projections. Proc. Intl. Soc. Mag. Reson. Med. 25 (2017)
7. Scheffler, K. & Hennig, J. Reduced circular field-of-view imaging. Magn. Reson. Med. 40, 474–480 (1998)
Figures