1472
Evaluation of RF-related heating of an MR-compatible catheter using MR-Thermometry1IHU Liryc, Electrophysiology and Heart Modeling Institute, Fondation Bordeaux Université, Bordeaux, France, 2Univ. Bordeaux, Centre de recherche Cardio-Thoracique de Bordeaux, U1045, Bordeaux, France, 3INSERM, Centre de recherche Cardio-Thoracique de Bordeaux, U1045, Bordeaux, France, 4Siemens Healthineers, Saint-Denis, France, 5Image Guided Therapy SA, Bordeaux, France
Synopsis
This study presents a fast MR-thermometry sequence interleaved with a tunable SAR deposition module to simulate energy deposition of any clinically relevant MR-acquisition sequence. Validation of the method was performed on a 1.5T scanner using an MR-compatible catheter inserted into an agar-agar gel. Maximal temperature increase measured during equivalent SAR of a cardiac cine sequence was 41.8°C for a 90° flip angle. This sequence may help quantifying the maximal acceptable SAR for any patient wearing implanted device and/or for volumetric imaging of local heating in multi-transmit technology at high field.
Introduction
A number of patients suffering from cardiac electrical disorders are implanted with stimulation devices or treated by heart catheterization. Magnetic Resonance Imaging is a method of choice for diagnosis and guidance of therapies. However, electromagnetic coupling between high power emission of the excitation pulses of each MRI sequence and the wires of the therapeutic devices or the metallic tip of a catheter may result in unwanted local tissue heating which can turn into unwanted adverse effects such as fibrillation or local thermal necrosis. Current safety studies mainly rely on in vitro invasive measurement using fiber-optic probes [1, 2]. However, this single point measurement does not provide spatial mapping of temperature distribution and cannot be applied in patients. MR-thermometry imaging methods have been proposed [3, 4] but are currently not fast enough for mapping temperature distribution in real-time in the heart. The purpose of this study is to develop a fast MR-thermometry sequence adapted to cardiac MR thermometry incorporating an adjustable energy deposition module interleaved with temperature imaging of the heart in real-time, in order to quantify the potential heating induced by sequences used for clinical diagnosis. Validation of the method was performed on a gel using a bipolar MR-compatible catheter.Materials and Methods
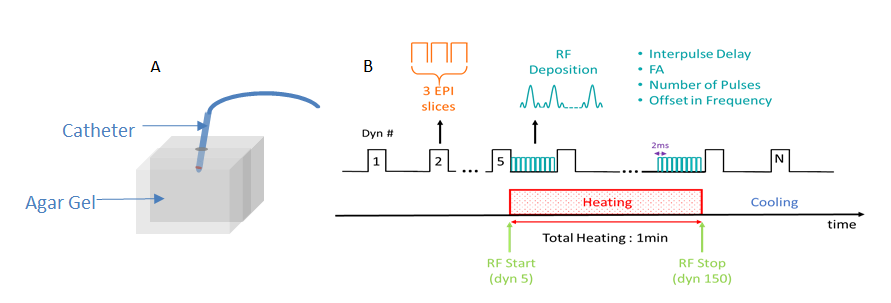
Experiments were performed on a clinical 1.5T scanner (Avanto, Siemens, Erlangen). An MR-compatible ablation catheter was inserted into an agar-agar gel, perpendicularly to static magnetic field and positioned at the MRI isocenter (Figure 1,A). The acquisition sequence was modified from an already published fast multislice sequence allowing cardiac thermometry [5]: a single shot Gradient Echo EPI acquisition was interleaved with a train of RF pulses with adjustable duration, flip angle, interpulse delay and number of pulses (Figure 2,B). Each RF pulse was emitted with a tunable frequency offset (typically 5 KHz) to avoid proton signal saturation on MR-temperature images [3]. For test purposes, the SAR of a cine true FISP imaging sequence was simulated using 2ms pulse duration, flip angle tuned between 0° and 90° by steps of 10° in separate measurements, and 200 consecutive trains between consecutive EPI imaging (TE/TR = 16 / 600 ms, FOV 180 mm, 1.6 mm voxel size, GRAPPA acceleration factor of 2, 75% partial Fourier) with 3 slices in transversal orientation centered on the catheter tip. Energy deposition module was activated during the first 150 repetitions followed by an off period to observe cooling.Results
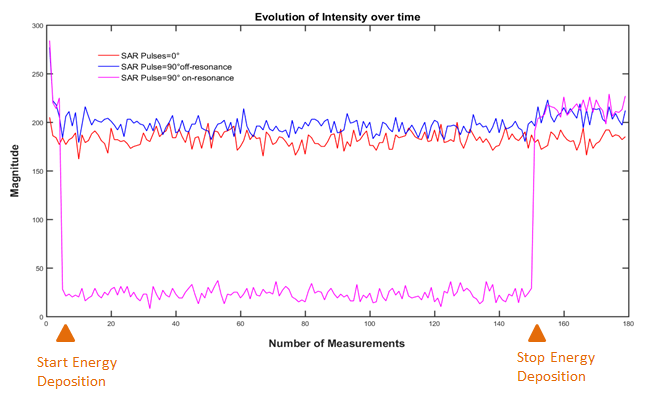
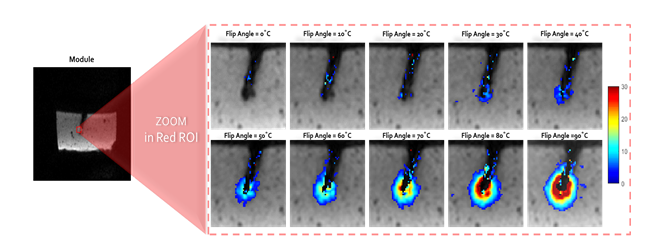
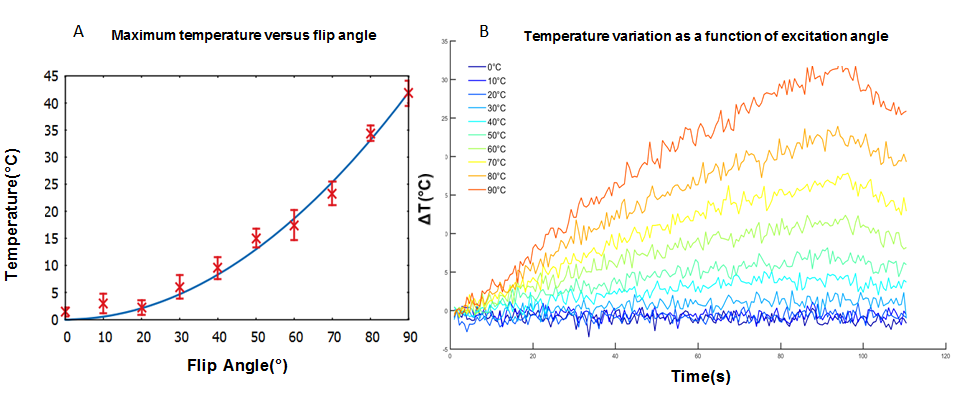
The off-resonant RF pulse allowed deposition of RF energy while keeping an SNR comparable with an EPI sequence acquired without RF energy deposition (Figure 2). MR-Thermometry was successfully monitored near the catheter tip with a mean temporal standard deviation below 1°C in absence of energy deposition over the entire gel. The standard deviation of the temperature in regions located in the gel but far away from the catheter tip were similar before and during RF energy deposition, indicative of no direct heating of the gel from the MR sequence itself. Figure 3 shows temperature maps derived for every acquisition. Maximal temperature increases were [1.4, 3, 2.2, 6, 9.5, 15, 17.4, 23.3, 34.4, 41.8]°C for flip angles ranging from [0° to 90° with 10° step], respectively. The temperature increase showed a quadratic evolution when plotted versus flip angle (T=a.(flip angle)² with a=5.2 10-3, R2= 0,991) (Figure 4, A).Discussion and conclusion
The developed MR-acquisition sequence provides a non-invasive method for imaging the temperature distribution near an implanted device for any clinically relevant MR acquisition sequence. This method may thus help quantifying the maximal acceptable Specific Absorption Rate (SAR) for each cardiac MR acquisition sequence to be applied for a given patient wearing implantable device to guaranty safety. Since the sequence is fast and multi-slice, other potential application of this method include definition of effective SAR deposition at high field when multiple transmit technology is required. The time penalty of the proposed sequence is reasonable (around 3 minutes) and can thus be included at the beginning of any MR examination protocol for calibration purposes.Acknowledgements
This work received financial support from the French National Investments for the Future Programs: ANR-10-IAHU-04 (IHU Liryc) and Laboratory of Excellence ANR-10-LABX-57 (TRAIL), and the research programs ANR-11-TecSan-003-01 (TACIT) and Equipex ANR-11-EQPX-0030 (MUSIC).References
[1] Nordbeck et al, Magnetic Resonance in Medicine 61:570-578 (2009)
[2] Armenean et al, Magnetic Resonance in Medicine 52:1200-1206 (2004)
[3] D.Gensler et al, Magnetic Resonance in Medicine 68:1593-1599 (2012)
[4] P.Ehses et al, Magnetic Resonance in Medicine 60:457– 461 (2008)
[5] V.Ozenne et al, Magnetic Resonance in Medicine 77:673–683 (2017)
Figures