1424
MRI findings in Early Rheumatoid Arthritis, their clinical correlate and method of assessment1Imaging and Interventional Radiology, The Chinese University of Hong Kong, Hong Kong, Hong Kong, 2Jockey Club Centre for Osteoporosis Care and Control, The Chinese University of Hong Kong, Hong Kong, Hong Kong, 3Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong, Hong Kong
Synopsis
This study investigated the correlation between MRI parameters and clinical assessment in 106 treatment naïve patients presenting with early rheumatoid arthritis (ERA) i.e. symptoms < 24 months. The degree of synovial and tenosynovial proliferation, bone marrow oedema and bone erosions were semi-quantitatively and quantitatively measured on MR imaging. Quantitative MRI parameters showed better correlation with clinical assessment than semi-quantitative methods. Only quantitative MRI methods showed significant change after treatment for one year.
INTRODUCTION
To determine if MRI features of inflammation correlate with clinical/serological features and what quantification method of assessment provides the best correlation at baseline and after one year of disease modifying anti-rheumatic drug treatment.METHODS
106 patients (81 females, 25 males, mean age, 53±12 years) with early (i.e. symptoms < 24 months) RA underwent clinical / serological testing as well as 3T dynamic contrast-enhanced (DCE) MRI of the most symptomatic wrist. Sequences obtained were: fat-saturated T1-weighted axial; fat-saturated T2-weighted coronal; T1-weighted coronal and dynamic fat-saturated post-contrast T1-weighted axial imaging. Analyses undertaken included:
1. Clinical / serological assessment (Health Assessment Questionnaire (HAQ), Physician Global Assessment (PGA), Simple Disease Activity Index (SDAI); erythrocyte sedimentation rate, C-reactive protein.
2. Semi-quantitative grading of (a) synovial proliferation (RAMRIS) and (b) tenosynovitis.
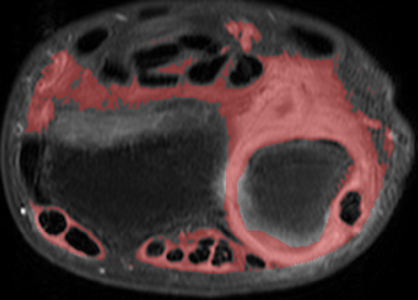
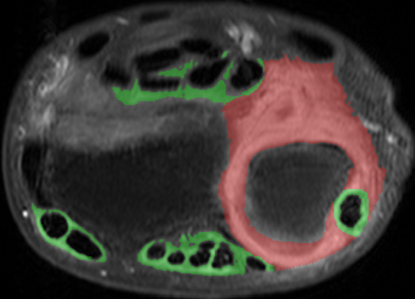
3. Quantitative measurement of enhancing synovial / tenosynovial volume (cm3) (Figure 1).
4. Maximum enhancement (Emax) and enhancement slope (Eslope) of enhancing synovium. Parameters were assessed at baseline and at one year follow up. Clinical / serological parameters were compared with MR parameters using Spearman’s correlation.
RESULTS
Synovitis was present in 104 (98%), bone marrow edema in 77 (73%), erosions in 87 (82%) and tenoynovitis in 82 (77%) of the 106 ERA wrists at presentation. For all analyses, clinical / serological parameters correlated better with quantitative than semi-quantitative parameters. Clinical characteristics namely PGA (r= 0.459, p<0.001), SDAI (r=0.414, p<0.00) and HAQ (r=0.300, p=0.004) correlated best with total synovial / tenosynovial volume while serological parameters ESR (r=0.403, p<0.001) and CRP (r=0.409, p<0.001) correlated better with perfusion parameters (Emax). Only quantitative measurements showed significant change at one year in line with clinical improvement. Both RAMRIS system or tenosynovitis grading failed to show any change at one year.CONCLUSION
Quantitative assessment of inflammatory change in ERA on MRI is much better than semiquantitative assessment. Clinical characteristics correlate more with synovial volume while serological characteristics correlate with perfusion parameters. Only quantitative measures, and not semiquantitative grading (RAMRIS and tenosynovitis grading), showed significant change at one year.Acknowledgements
No acknowledgement found.References
No reference found.Figures