1380
Comparison of T2 Relaxation Times in Knee Cartilage Between Breaststroke and Nonbreaststroke Swimmers1Radiology, Stanford University, Stanford, CA, United States, 2Bioengineering, Stanford University, Stanford, CA, United States, 3Orthopaedic Surgery, Stanford University, Stanford, CA, United States
Synopsis
While MRI has been widely used to examine the effects of translational forces on cartilage matrix structure, studies looking at rotational forces are limited. Breaststroke swimmers are a population of interest since the repeated use of the breaststroke kick has been cited as a source of knee pain. However, the cartilage of breaststrokers has not been quantitatively measured to investigate possible differences and the potential increased risk of cartilage degeneration and osteoarthritis development. This study compares the T2 relaxation times of various compartments for patellar, femoral, and tibial cartilage at the superficial, deep, and aggregate levels between breaststrokers and nonbreaststrokers.
Purpose
Osteoarthritis (OA) is a degenerative disease of the joint1, which is expected to affect 25% of U.S. adult population by 20302. While MRI has been widely used to examine the effects of translational forces on cartilage matrix structure, studies looking at rotational forces are limited. Breaststroke swimmers provide an interesting population to evaluate the impact of high rotational forces on cartilage degeneration and knee pain. Additionally, they are a well-controlled group since there is minimal impact on their knees from swimming and activities outside of swimming. Breaststroke swimmers have been shown to have a high incidence of knee pain, likely as a result of the demanding biomechanics of the breaststroke kick, where the knee goes from flexion to extension with a valgus stress and external rotation3 (Fig. 1). Competitive breaststrokers who had used the kick for more than 8 years had clinical evidence of patellofemoral osteoarthritis4. T2 relaxation time mapping, a quantitative MRI measure, can provide an objective assessment of early changes in cartilage hydration or matrix structure in this population5. The aim of this study is to determine if there are quantitative differences in the T2 relaxation times for knee cartilage between breaststrokers and nonbreaststrokers, which may indicate an increased risk of developing osteoarthritis.Methods
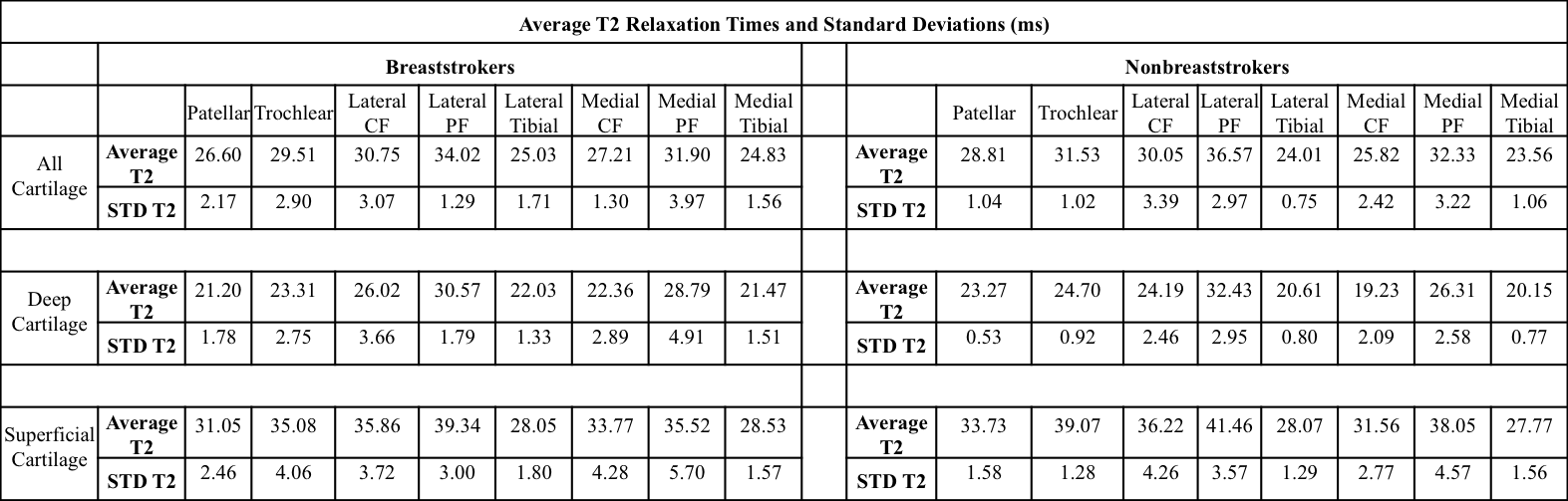
Six breaststrokers’ knees (from 3 subjects) and four nonbreaststrokers’ knees (from 3 subjects) were scanned on a 3.0T scanner (GE Healthcare) using 16-channel flex knee coil-arrays. All subjects were elite swimmers (Division 1 college or higher) who did not participate in other sports and had no history of knee pain or injury in either knee. Breaststrokers were identified if more than 20% of the swimming distance in their swimming workouts was done as breaststroke while nonbreaststrokers were defined as having less than 20% of their swimming distance completed as breaststroke. A quantitative double-echo in steady-state (DESS) sequence was used for image acquisition (FOV=16 cm, matrix=384x384, TR/TE1/TE2 = 14.4/4.9/23.8 ms) from which T2 relaxation time mapping was performed by fitting the two qDESS images to complex signal models6. For each subject, 8 cartilage compartments across the patellar, femoral, and tibial cartilage were manually segmented using the morphological DESS images, and T2 relaxation times for all cartilage, deep layer cartilage, and superficial layer cartilage were extracted (Table 1). T2 values for all cartilage compartments were compared between breaststrokers and nonbreaststrokers using a Wilcoxon Rank-Sum Test.Results & Discussion
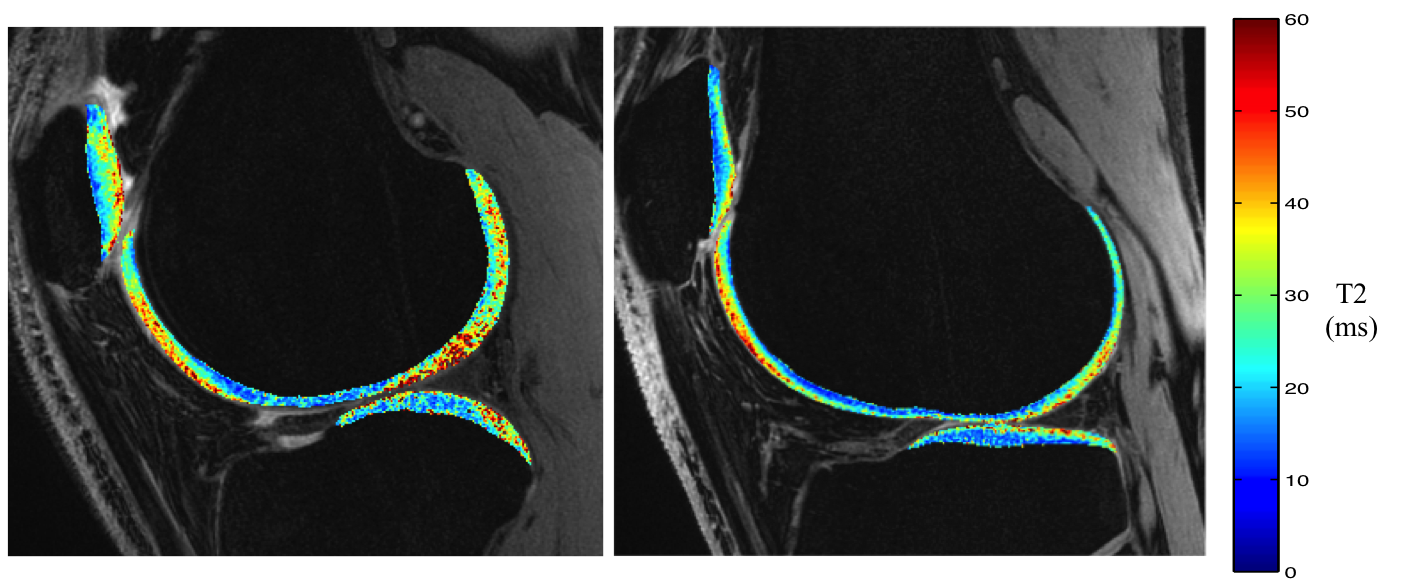
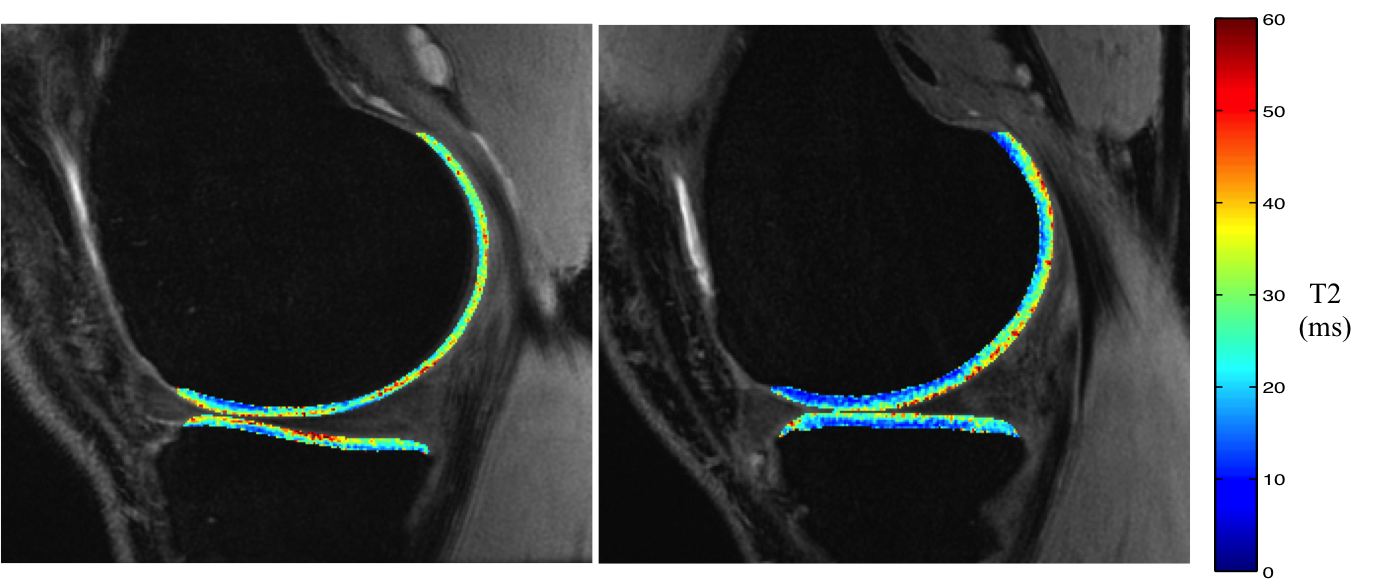
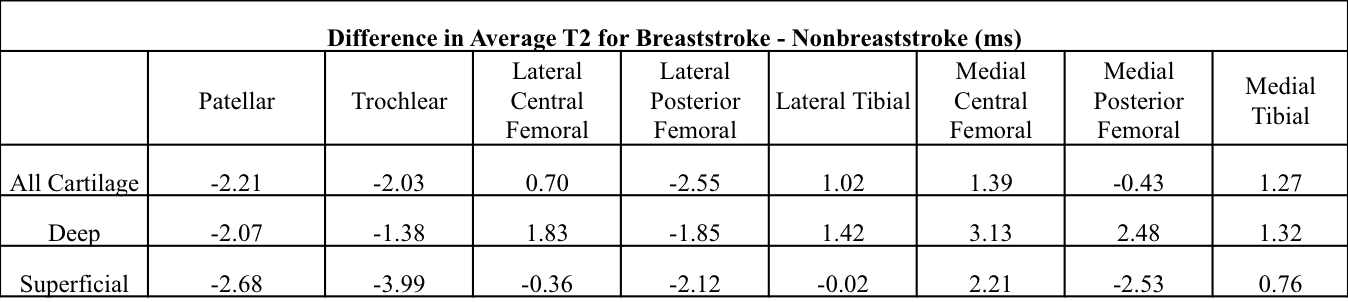
Figure 2 and Figure 3 show representative T2 relaxation time maps of the lateral and medial knee compartments, respectively, for a breaststroker knee and a nonbreaststroker knee. Breaststrokers had lower mean T2 values than nonbreaststrokers for all cartilage, deep cartilage, and superficial cartilage within the patellar and trochlear cartilage regions (Tables 1 & 2). On the other hand, it is noteworthy that breaststrokers had elevated mean T2 values compared to nonbreaststrokers for all cartilage as well as within both deep and superficial layers of cartilage within the medial central femoral and medial tibial regions (Tables 1 & 2) since the most common site of breaststroke knee pain is the medial portion of the knee7. However, the limited sample size did not provide sufficient power to determine significant differences between the T2 values of breaststrokers and nonbreaststrokers in any of the compartments analyzed. Further studies are ongoing to increase the study size as well as to evaluate other quantitative MRI measures of cartilage and other joint tissues. In particular, the effects of high rotational forces on the meniscus and the medial collateral ligament (MCL) are of interest, as injuries to these tissues have been linked to the repeated use of the breaststroke kick8.Conclusion
Although no significant differences were found, higher T2 relaxation times were observed in the medial central femoral and medial tibial regions of breaststroke swimmers compared to nonbreaststroke swimmers (Tables 1 & 2). Larger studies are ongoing to further evaluate the significance of rotational forces on early cartilage matrix changes in these elite-level athletes.Acknowledgements
This work was funded by GE Healthcare and National Institute of Health (NIH) grants R01EB002524, R01AR0063643, K99EB022634, and K24AR062068.References
1. Braun H. J., Gold G. E. Diagnosis of osteoarthritis: imaging. Bone. 2012; 51(2):278–288. doi: 10.1016/j.bone. 2011.11.019.
2. Hootman JM, Helmick CG. Projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum. 2006; 54:226-9.
3. Kennedy JC Hawkins R Krissoff WB. Orthopeadic manifestations of swimming. Am J Sports Med. 1978;6:309-322.
4. D. Stulberg, K. Shulman, S. Stuart, P. Culp. Breaststroker's knee: pathology, etiology, and treatment. The American Journal of Sports Medicine. 1980:8(3):164-171. 10.1177/036354658000800304
5. Mosher TJ, Dardzinski BJ. Cartilage MRI T2 relaxation time mapping: overview and applications.Semin Musculoskelet Radiol. 2004;8:355–368.
6. Sveinsson B, Chaudhari AS, Gold GE, Hargreaves BA. A simple analytic method for estimating T2 in the knee from DESS. Magn Reson Imaging 2017;38:63-70.
7. Rovere GD, Nichols AW. Frequency associated factors and treatment of breaststrokers’ knee in competitive swimmers. Am J Sports Med. 1985;13:99–104.
8. S Kammer, C & C Young, C & Niedfeldt, Mark. (1999). Swimming Injuries and Illnesses. The Physician and sportsmedicine. 27. 51-60. 10.3810/psm.1999.04.783.
9. Swimming : - breaststroke kick drills. (n.d.). Retrieved from https://www.nataswim.info/swimming-online-coaching/6782-breaststroke-kick-drills
Figures
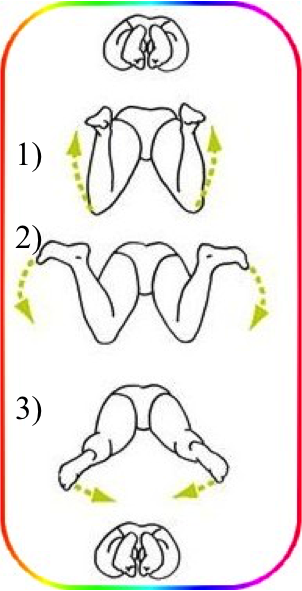
Figure 1: Breaststroke kick mechanics9
1) Flexion of the knee joint
2 & 3) extension with valgus stress and external rotation causing high rotational force on the medial part of the knee