1317
The Effect of B0 and B1+ Inhomogeneities on Spinal Cord MRS1School of Biomedical Engineering, McMaster University, Hamilton, ON, Canada, 2Department of Kinesiology, McMaster University, Hamilton, ON, Canada, 3Department of Electrical and Computer Engineering, McMaster University, Hamilton, ON, Canada
Synopsis
Spinal cord 1H MR Spectroscopy (1H-MRS) is a promising method for musculoskeletal research. However, due to the spine’s anatomical location there is a significant degradation of signal quality due to magnetic field inhomogeneities, rendering most MRS approaches inaccurate. Although there has been measurement of ΔB0 in spinal cord MRS, there are no comprehensive assessments of temporal changes in B0 and B1+ relating physiological disturbances with MRS accuracy. Thus our goal was to continually measure temporal changes in B0 and B1+ during the length of a typical MEGA-PRESS scan (10min).
Introduction
Spinal cord 1H MR Spectroscopy (1H-MRS) is a valuable non-invasive tool that can provide insight into the biochemistry of tissue-specific metabolites. As such, investigation in the cervical spinal cord is a promising area of research and clinical study due to its functional involvement in the upper limb. However, due to a variety of technical challenges due to the spinal cord’s anatomical location, there is significant degradation of signal quality by magnetic field inhomogeneities and pulsatile and respiratory motion rendering most MRS approaches 1. Although there have been measurements and protocols to identify B0 and B1+ field changes in spinal cord MRS 2 there have not been ay comprehensive and quantitative assessments of temporal changes that could occur during the length of a typical MRS protocol. Therefore, our goal was to measure contiguous temporal changes in B0 and B1+ 3 during the length of a typical MEGA-PRESS scan, while recording physiological data, to quantify the impact of their variability in spinal cord MRS.Methods
Experiments were performed using a 3T GE MR750 scanner and a 32 channel receive-only
head/neck array RF coil (General Electric Healthcare, Milwaukee, WI). Measurements were made on a static home
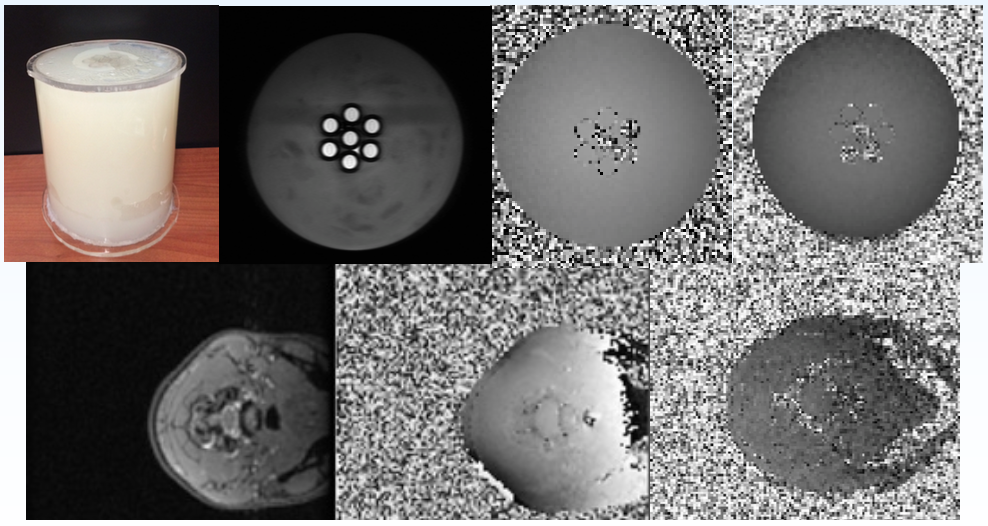
designed/built spinal cord phantom and a healthy human subject. In separate experiments B0 and B1+ field maps were repeatedly acquired over a 10 minute timespan in the phantom and
cervical spinal cord (C4) of a human subject (Fig.1). The B0 and B1+ sequences,
each taking 6s
and 11s respectively, were
auto-shimmed only for the first measurements so the same shim currents were
maintained for the duration of the 10 minutes. Acquisition of heart rate and respiration were
performed using a pulsed oximeter and thoracic respiratory bellows, both temporally
synchronized with the beginning of the first scan. These were continually recorded over the
length of the 10 minute scan at a sampling rate of 10Hz and 25Hz, respectively.
Results and Discussion
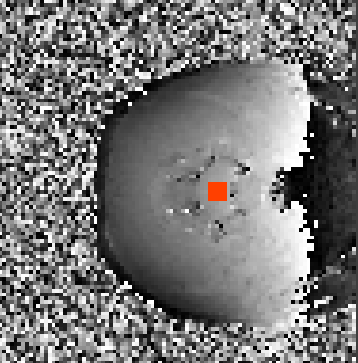
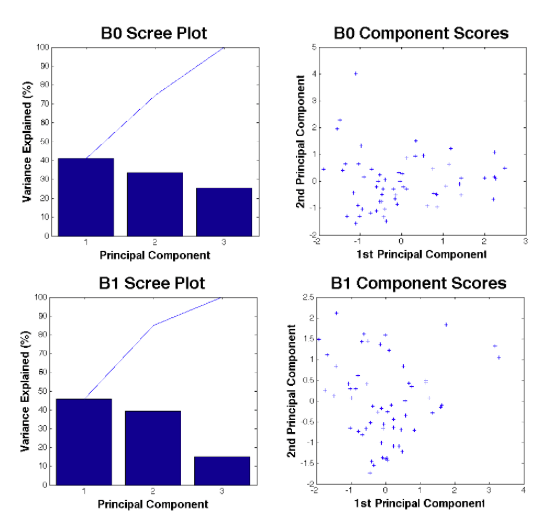
ROIs were selected in B0 and B1+ field maps of the spinal cord phantom and human C-spine (Fig.2) and means and standard deviations were calculated. There was slight variation in the B0 (mean±SD) 60.7±0.51Hz and B1+ 28.4±2.72 degrees/flip angle fields within the spinal cord, over the 10minutes of scanning. Whereas there was significant variation in the B0 (mean±SD) 48.5±2.72Hz and B1+ 21.4±4.61 degrees/flip angle fields within the spinal cord, over the 10minutes of scanning. Hence, physiological variation was more the dominant contribution to variability. The heart rate data was Fourier transformed (FT) and the power spectral density (PSD) was used to identify the dominant frequency contribution of motion for each field map. A standard deviation window for each field map was found for the respiratory motion contribution. The physiological data was further analyzed using principal component analysis (PCA) (Fig.3). The dominant principal component in B0 variability, heart rate, yielded a correlation coefficient of 0.71 whereas for B1+, the dominant principal component, respiratory motion, yielded a correlation coefficient of 0.52.
Conclusions
There are significant links between physiological data and inhomogeneities of B0 and B1+ within the spinal cord. For spinal cord MRS, gating techniques should be emplyed to reduce cardiac and respiratory effects. In addition, further exploration into the relationship between the B0 and B1+ magnetic field changes and respiratory/cardiac motion are needed to establish a difference equation that can further reduce physiological noise within spinal cord data acquisition. Further research should include larger sample sizes, slice position checks, and more component variables such as water peak centre frequency, shim, and MR noise.Acknowledgements
Special Thanks to Michael D. Noseworthy's guidance, Norm Konyer's abilities, and Diana Harasym and Alejandro Santos Diaz's continued supportReferences
[1] Henning A., et al. (2008) Magn Reson Med 59(6):1250-1258.
[2] Cooke FJ. et al (2004) Magn Reson Med 51(6):1122-1128.
[3] Sacolick Li. et al. (2010) Magn Reson Med 63(5):1315-1322.
Figures