1248
Zero TE Hip MRI: Osseous Measurements Assessing Femoroacetabular Impingement1Radiology and Imaging, Hospital for Special Surgery, New York, NY, United States, 2Sports Medicine, Hospital for Special Surgery, New York, NY, United States
Synopsis
Due to short tissue relaxation times and signal scarcity, routine MRI does not provide direct visualization of bone. This study investigates the use of proton density zero echo time (ZTE) MRI of bone in the hip, with emphasis on femoroacetabular impingement (FAI). Hip CT and ZTE images were acquired for 24 hips (14 patients). Ten measures of osseous morphology were compared between modalities. 'Moderate' to 'excellent' agreement was seen in all but one of the measurements. Zero Echo Time MRI may mitigate the need for CT in some cases.
Introduction
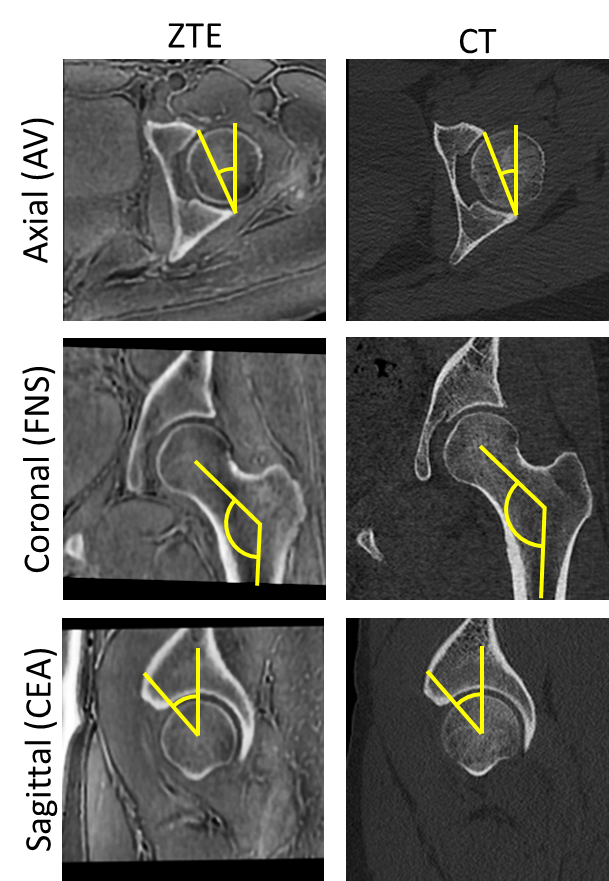
Femoroacetabular impingement (FAI), commonly defined as an intrusion of the femoral neck onto the acetabulum (cam impingement) or excessive coverage of the femur by the acetabulum (pincer impingement), requires accurate osseous imaging of the hip to characterize the severity of the condition and to determine the appropriate course of treatment. MRI is commonly employed to assess concomitant soft tissue injury, but does not provide direct visualization of the impinging bone due to the tissue's inherent short transverse relaxation time and limited signal intensity. Zero echo time (ZTE) MRI enables visualization of bone with CT-like contrast1,2, figure 1. Clinical application of ZTE imaging has been explored in the cranium2, as well as the shoulder3 and spine4 but has not yet been applied to the hip2. The objective of this study was to investigate whether ZTE MRI of the hip, in the setting of FAI, permits sufficient visualization of bone when compared to a CT gold standard.Methods
As part of a larger IRB-approved study, a subset of 24 hips from 14 patients (11F/3M; 26.8±9.7 y.o.; mean±SD) were selected and consented/assented for participation, yielding a total of 11 hips. Patients were included based on scheduled or existing CT scans (< 12 mo. from MRI) with no intervening surgery altering the osseous hip morphology. Following institutional standard-of-care hip MRI examination, an axial ZTE hip series was acquired with the following parameters: TR: 300ms, flip angle: 1°, receiver bandwidth: ±62.5 kHz, matrix size: 320, slice thickness: 1.2-1.5 mm, scan time: ~4-6 mins. MRI scanning was performed on clinical 3.0T scanners (Discovery MR750, GE Healthcare, Waukesha, WI). Standard patient positioning and commercial, 8-channel cardiac or 32-channel body coils were used for all imaging. Sagittal, coronal, and radial (about the femoral neck axis) reconstructions of the axial CT and ZTE were generated, and used for measurements. Measurements included: alpha and beta angles, denoting the angular extent of the femoral head and acetabulum in the anterior direction, respectively; coronal and sagittal center-edge angles (C-CEA, S-CEA), denoting the extent of the acetabulae; Tönnis angle5; and acetabular version at 3 different depths in the axial reconstruction (corresponding to clock-face locations of 1, 2, and 3 o’clock). Radiology technologists performed the multiplanar reconstructions and FAI measurements which were subsequently reviewed by a board-certified radiologist. Intraclass correlation coefficients (ICC) were used to quantify the agreement between measurements made on CT and ZTE.
Results
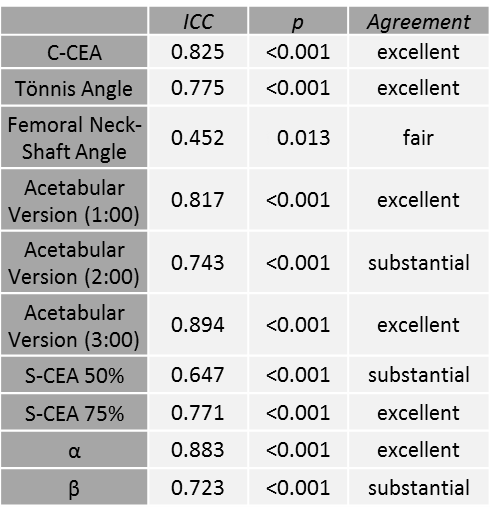
ZTE MRI produced images with osseous detail sufficient for the performance of all measurements. Intraclass correlation coefficients indicated substantial (ICC > 0.60) to excellent (ICC > 0.75) agreement for all FAI measurements except femoral neck shaft angle, which exhibited ‘fair’ agreement (ICC = 0.452), Table 1.Discussion
This study performed a one-to-one comparison of bony morphologic measurements between ZTE MRI and gold standard CT images. Nearly all measurements had substantial to excellent agreement. The weaker concordance of the femoral neck-shaft angle is likely an artifact of the approximation of the slice location used for this measurement and not the result of true discrepancies in the images. Additionally, some variation exists in the hip joint posture between modalities which further may account for some of the differences observed in each measurement.Conclusion
Visualization of bony detail is essential for diagnosis of FAI. FAI commonly injures the labrum and other soft tissues and patients routinely undergo MRI examination as these tissues are not well-visualized on CT. The concordance of measurements taken from ZTE MRI in the current study suggest that CT evaluation, with its attendant ionizing radiation, may be avoided for morphologic measurements used to diagnose FAI. ZTE MRI uses no ionizing radiation and affords isotropic acquisitions, amenable to multiplanar reformatting required for oblique measurements such as these. Further evaluation of this imaging technique in a larger cohort of FAI patients is currently underway.Acknowledgements
The authors wish to acknowledge HSS Radiology and Imaging CT technologists for assistance with FAI measurements.
HSS maintains an institutional research agreement with GE Healthcare.
References
1. Delso G, Wiesinger F, Sacolick LI, et al. Clinical evaluation of zero-echo-time MR imaging for the segmentation of the skull. J Nucl Med. 2015.
2. Wiesinger F, Sacolick LI, Menini A, et al. Zero TE MR bone imaging in the head. Magn Reson Med. 2015.
3. Breighner RE, Endo Y, Konin GP, et al. Zero Echo Time Imaging of the Shoulder: Enhanced Osseous Detail Using MRI. Radiology 2018; in press.
4. Argentieri EC, Koff MF, Breighner RE, et al. Diagnostic Accuracy of Zero-Echo Time MR Imaging for the evaluation of cervical neural foraminal stenosis. Spine. 2017; epub.
5.Beltran LS, Rosenberg ZS, Mayo JD, et al. Imaging evaluation of developmental hip dysplasia in the young adult. AJR Am J Roentgenol. 2013.
Figures