1228
Characterization of Ultra-short Echo and Standard echo Phase-Contrast MRI for Neurovascular disease applicationDahan Kim1,2, Katrina Ruedinger3, David Rutkowski3, Alejandro Roldán-Alzate4,5, Patrick Turski2,5, and Kevin M Johnson2,5
1Department of Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Department of Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 3Department of Biomedical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 4Department of Mechanical Engineering, University of Wisconsin - Madison, Madison, WI, United States, 5Department of Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
We examined velocity measurements of standard (STD-PC) and ultra-short echo (UTE-PC) phase-contrast MRI in three different study cases, to characterize the effect of shortening echo time on artifacts from flow and metal. We found that UTE-PC measures higher velocity magnitudes not only in disturbed flow but also in normal vasculature, that UTE-PC results in smaller divergence of velocity field but no difference in erroneous flux through arterial wall within metal aneurysm stent, and that UTE-PC higher velocity magnitudes, less signal loss, and coherent flow directions in both untreated and un-treated aneurysm phantom.
Introduction
Artifacts from flow and metal are often sensitive to echo time and by shortening the echo time (TE) intra-voxel dephasing based artifacts can be reduced. For 4D-flow imaging, the shortest possible echo times can be achieved using center out 3D radial sampling1, so called ultra-short echo time phase contrast (UTE-PC). Unfortunately, center-out radial also has lower sampling efficiency and higher noise than other radial and Cartesian sampling strategies. Hence, UTE-PC may result in degraded image quality in areas without disturbed flow, metal devices, or disturbed flow. The general consistency between STD-PC and UTE-PC has not been well characterized in clinical intracranial scans or in the presence of metal. In this work, we compared STD-PC and UTE-PC in three different study cases, and intended to assess the accuracy of each technique with different data fidelity measures.Methods
Using a 3T scanner (MR750, GE Healthcare, WI, USA) with a 32-channel head coil (Nova Medical, MA, USA), standard echo (STD-PC) and ultra-short echo (UTE-PC) phase-contrast MRI were performed in (1) seven human subjects with known neurovascular disease, (2) a patient treated with a stent for intracranial aneurysm, and (3) two patient specific intracranial aneurysm phantoms, one untreated and the other pseudo-treated with endovascular coiling. Both scans were acquired with 3D radial sequences1,2 with 0.6mm isotropic spatial resolution, and were registered (3D, rigid) to each other using their magnitude images with a mutual information metric (ANTs)4. For (1), both STD-PC and UTE-PC were reconstructed using standard (STD) and iterative compressed sensing (CS) reconstructions. Flow vectors were compared voxel-wise between STD-PC and UTE-PC for blood vessels over the whole brain, identified with a manual threshold in the PC-derived angiogram (PC-MRA). For (2), STD-PC and UTE-PC were assessed for self-consistency using the following two measures: (i)divergence of velocity fields, normalized to flow magnitudes, and (ii)flux of blood flow through the vessel wall. The through-wall blood flux was calculated by taking the dot-product between interpolated velocity vectors at the vessel wall and normal vectors at the vessel wall surface, evaluated over all surface area elements in the surface mesh of the segmented vessel. For (3), the two phantoms were connected in series and imaged side-by-side using a flow pump at steady flow rate 0.5L/min.Results
Comparison between STD-PC and UTE-PC from the 7 subjects shows that UTE-PC measures higher velocity than STD-PC on the average (Fig.1a-b), when examined over the entire vasculature of the brain. Compressed sensing (CS) did not change that trend or the magnitude of the disagreement between the two techniques. When each of STD-PC and UTE-PC were compared with itself between standard (STD) and CS reconstructions(Fig.2a-b), CS also did not make any meaningful difference in the flow values of PC-MRI. STD-PC and UTE-PC shows an excellent agreement in the flow directions, in both STD and CS reconstructions. Divergence of flow vectors, normalized relative to the flow magnitude, was higher within the metal stent, which is the area of signal loss, compared to the volume outside the stent(Fig.2). Within the stent, the normalized divergence was lower in UTE-PC than in STD-PC, indicating greater self-consistency of UTE-PC in its flow values. When the blood flux was calculated through the stent wall, there was no meaningful difference between STD-PC and UTE-PC, despite both having higher flux within the stent than outside the stent(Fig.4) . UTE-PC in the aneurysm phantoms are characterized with more homogeneous signal, higher velocity magnitudes, and directions in agreement with general flow. STD-PC shows areas of signal loss near both the treated(Fig.5b) and untreated(Fig.5d) aneurysms.Discussion/Conclusion
Although shortening TE has been shown to reduce flow artifacts in stenotic phantoms5,6, we find it true even when the entire cerebral vasculature was examined, not just the areas of disturbed flow. Divergence must be zero for a completely accurate measurement of velocity field of blood, and was used here as a metric to assess the accuracy of velocity measurements, without reference to ground truth. We found lower divergence in UTE-PC than STD-PC, and that UTE-PC yields more self-consistent velocity fields. Since macroscopic blood flow does not occur through the arterial vessel wall, we computed the through-wall flux as a measure of velocity field accuracy. However, we did not find any meaningful difference with this metric between UTE-PC and STD-PC in the stent examined, especially with the signal loss in the area. Although UTE-PC showed higher velocity magnitudes, we could not characterize the effect of metal due to presence of disturbed blood flow, suggesting improved phantom design free of disturbed flow for future studies.Acknowledgements
No acknowledgement found.References
1. Johnson KM. 5-Point, Ultra-Short TE, 3D radial Phase Contrast: Improved characterization of Complex and Turbulent flow. 2010. Proc of 18th Meeting and Exhibition of the International Society for Magnetic Resonance in Medicine. Stockholm, Sweden. Abstract #66 2. Johnson KM, Lum DP, Turski PA, Block WF, Mistretta CA, Wieben O. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. Magn Reson Med. 2008;60(6):1329-1336. 3. Johnson KM, Fain SB, Schiebler ML, Nagle S. Optimized 3D Ultrashort Echo Time Pulmonary MRI. Magn Reson Med. 2013;70(5):1241–1250. 4. B.B. Avants, N.J. Tustison, G. Song, P.A. Cook, A. Klein, J.C. Gee. A reproducible evaluation of ANTs similarity metric performance in brain image registration. Neuroimage. 2011;54(3)2033-2044 5. O’Brien KR, Cowan BR, Jain M, Stewart RA, Kerr AJ, Young AA. MRIphase contrast velocity and flow errors in turbulent stenotic jets. JMagn Reson Imaging 2008;28:210–218.Figures
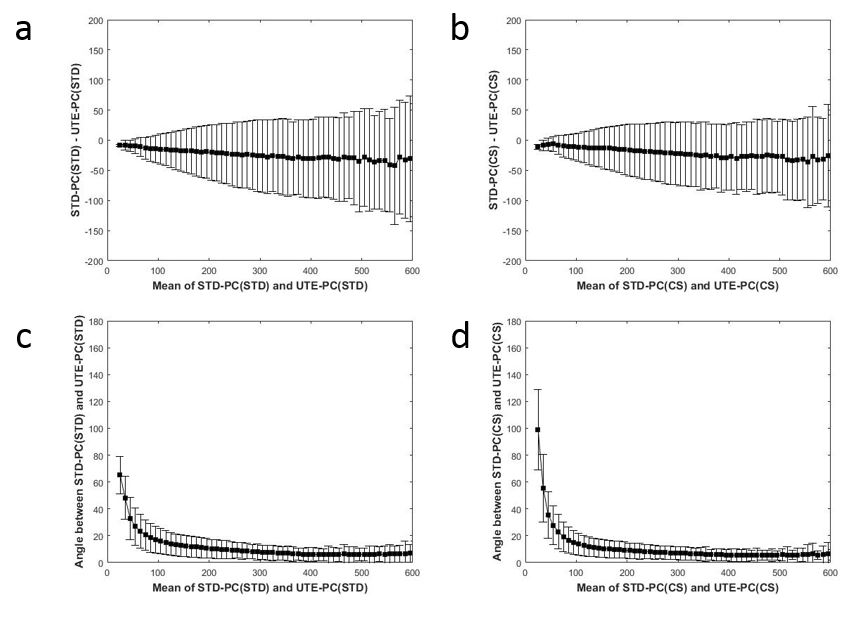
Figure 1. Bland-Altman plots comparing velocity magnitudes (a-b)
and angles (c-d) between STD-PC and UTE-PC. The left column (a and c) shows
comparison with standard (STD) reconstruction. The right column (b and d) shows
comparison with compressed sensing (CS) reconstruction.
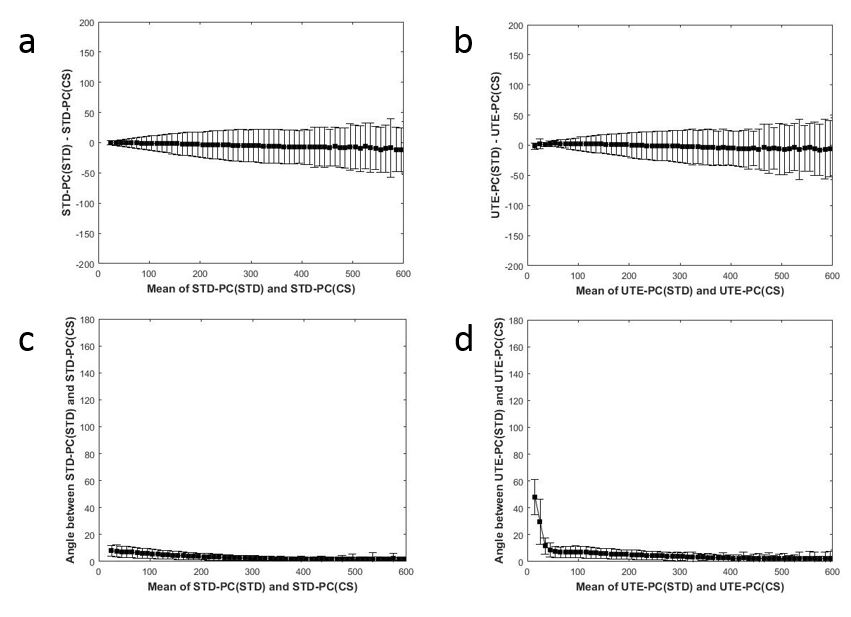
Figure 2. Bland-Altman plots comparing velocity magnitudes (a-b)
and angles (c-d) between standard (STD) and compressed sensing (CS)
reconstructions. The left column (a and c) shows comparison of STD-PC with
itself between STD and CS reconstructions. The right column (b and d) shows
comparison of UTE-PC with itself between STD and CS reconstructions.
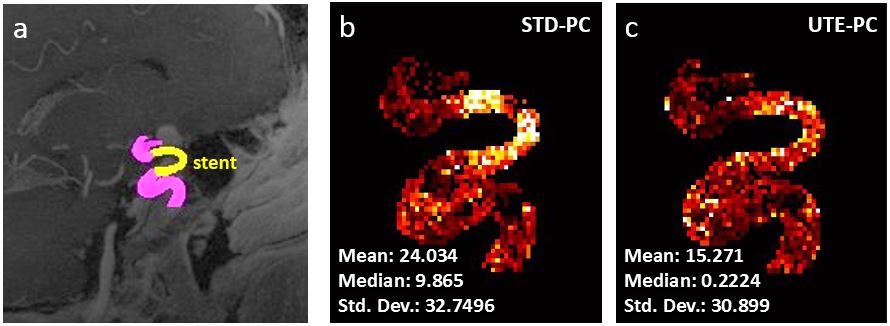
Figure 3. (a) UTE-PC magnitude image of a patient treated
with metal stent for intracranial aneurysm. Maximum-intensity projection (MIP)
of normalized divergence of velocity fields in (b) STE-PC and (c) UTE-PC, shown
with statistics for values within the stent only.
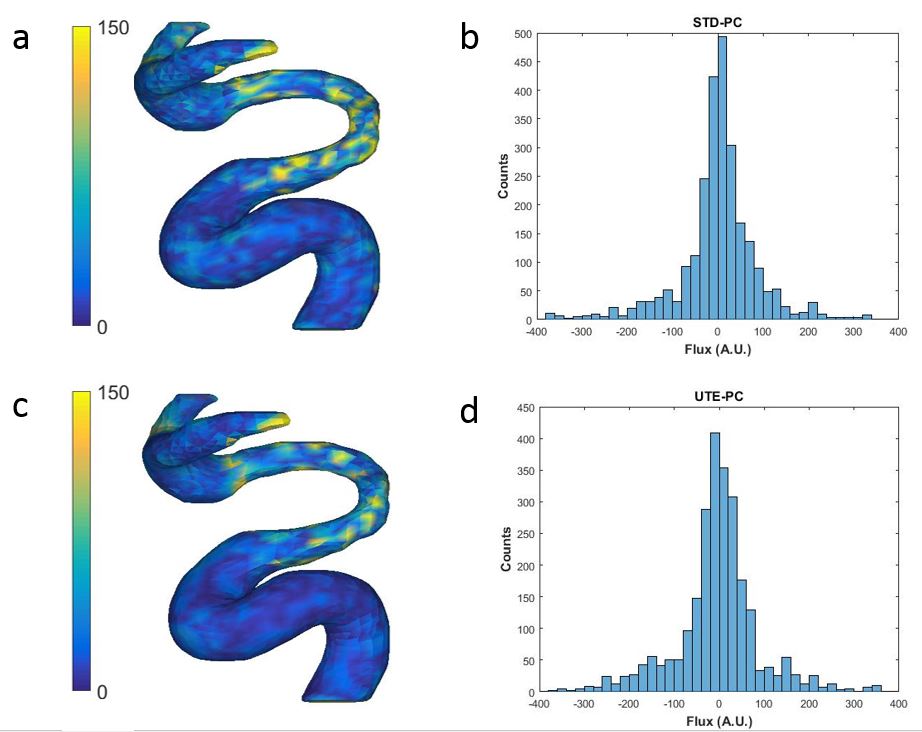
Figure 4. (a) Flux of blood flow through the vessel wall,
calculated from STD-PC velocity field. (b) Histogram of the through-wall blood
flux, calculated with STD-PC for surface area elements within the stent. (c)
Flux of blood flow through the vessel wall, calculated from UTE-PC velocity
field. (d) Histogram of the through-wall blood flux, calculated with UTE-PC for
surface area elements within the stent.
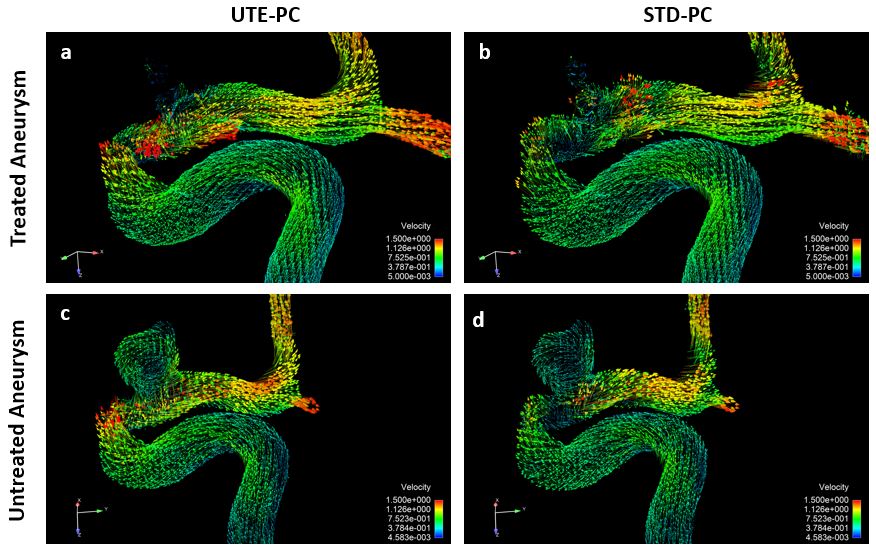
Figure 5. Comparison of STD-PC and UTE-PC in aneurysm
phantoms, (a-b) treated with endovascular coiling and (c-d) untreated.