1223
4D Flow assessment of arterial pulsation in the patients with internal carotid artery stenotic disease1Radiology, Nippon Medical School, Tokyo, Japan, 2Neurosurgery, Nippon Medical School, Tokyo, Japan, 3Radiology, Nihon University School of Medicine, Tokyo, Japan, 4Philips Electronics Japan, Tokyo, Japan
Synopsis
We performed 4D Flow MRI assessment of arterial pulsation in internal carotid artery stenotic disease (ICS) patients comparing to SPECT with acetazolamide challenge. Twelve patients with unilateral ICS were recruited. The blood flow volumes and the ratio of ΔF (rΔF) was calculated. In the affected-side MCA territory, the ratio of rest cerebral blood flow control (RCBFMCA) and cerebral vascular reserve (CVRMCA) were calculated from SPECT dataset. rΔF was significantly lower in the low CVR group than high group (P=0.008). The 6-min-standard 4D Flow MRI assessment of arterial pulsation in ICS patients can identify misery perfusion.
Introduction
Internal carotid artery stenotic disease (ICS) is a common condition in patients with atherosclerosis and considered a risk factor for cerebral ischemic event. In patients with ICS, a marginally adequate blood supply relative to metabolic demand (misery perfusion) in the affected hemisphere may increase the risk of cerebral ischemic event. To identify misery perfusion, positron emission tomography (PET) or single photon emission CT (SPECT) with acetazolamide challenge are used as gold standard (1). However, these measurements are not widely distributed clinically due to the cost, complexity of procedures and adverse event of acetazolamide. As alternative modalities, sonography and 2D phase-contrast MR imaging have been tried. The pulsation of artery derived from these modalities correlates to peripheral cerebral resistance which decreases to maintain adequate perfusion of the cerebral hemispheres in the patients with ICS (2). The limitation of these modalities may be necessity of skilled operators, narrow coverage of target lesion and low reproducibility. Recently, clinical MRI scanners have installed time-resolved 3D phase contrast (4D Flow) MRI. 4D Flow MRI is expected to make the measurement of arterial pulsation more objective and reliable by retrospective flow quantification from 3D imaging volume (3). The purpose of this study was to assess the feasibility of 4D Flow MRI assessment of arterial pulsation in ICS patients comparing to SPECT date with acetazolamide challenge.Materials and Methods
Patients; Twelve consecutive patients with unilateral ICS who underwent both 4D Flow MRI and acetazolamide-stress brain perfusion SPECT between January 2010 and November 2016 were retrospectively reviewed.
MRI Acquisition; 4D Flow MRI was performed using a 3.0-T MRI unit (Achieva; Philips Healthcare, Best, The Netherlands). The parameters were as follows: TR/TE 8.4/5.4 ms; k-space segmentation factor 2; temporal resolution 67.2 ms; flap angle (FA) 13°; velocity encoding (VENC) 100 cm/s (VENC range, 200cm/sec), voxel size 0.82×0.82×1.4mm3; 15 cardiac phases; SENSE factor2; elliptical partial k-space coverage in phase-and slice-encoding direction; and acquisition time approximately 6 min (4).
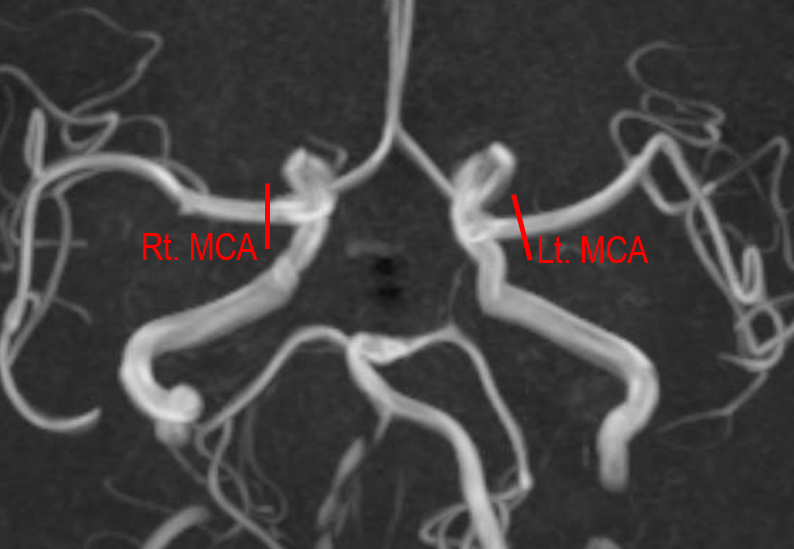
4D Flow MRI Analysis; We analyzed all data using GTFlow software (version 3.1.0, GyroTools, Zurich, Switzerland). 2D analysis planes were manually positioned vertical to long axis of vessels in M1 segment of MCA as shown in Fig. 1, using the magnitude images for anatomic orientation. For each analysis plane, ROI was placed on the vessels by using iso-contour method. The systolic and diastolic blood flow volume (BFV) (ml/sec) were measured. To measure arterial pulsation, the difference between systolic and diastolic BFV was defined as ΔF. The ratio of ΔF (rΔF) was calculated by dividing ΔF of affected side by that of contralateral side.
SPCET acquisition and analysis; All patients underwent acetazolamide-stress and rest 123I-IMP brain perfusion SPECT. Cerebral blood flow (CBF) was calculated using the autoradiography (ARG) method. In the affected-side MCA territory, the ratio of rest CBF to the default value obtained from healthy participants (RCBFMCA) were calculated. In addition, the cerebral vascular reserve in the affected-side MCA territory (CVRMCA) was calculated by dividing (stress CBF – rest CBF) by the rest CBF. According to previous study, patients were assigned to two groups as follows: 1) low CVR group and high CVR group, 2) low RCBF group and high RCBF group (5).
Restults
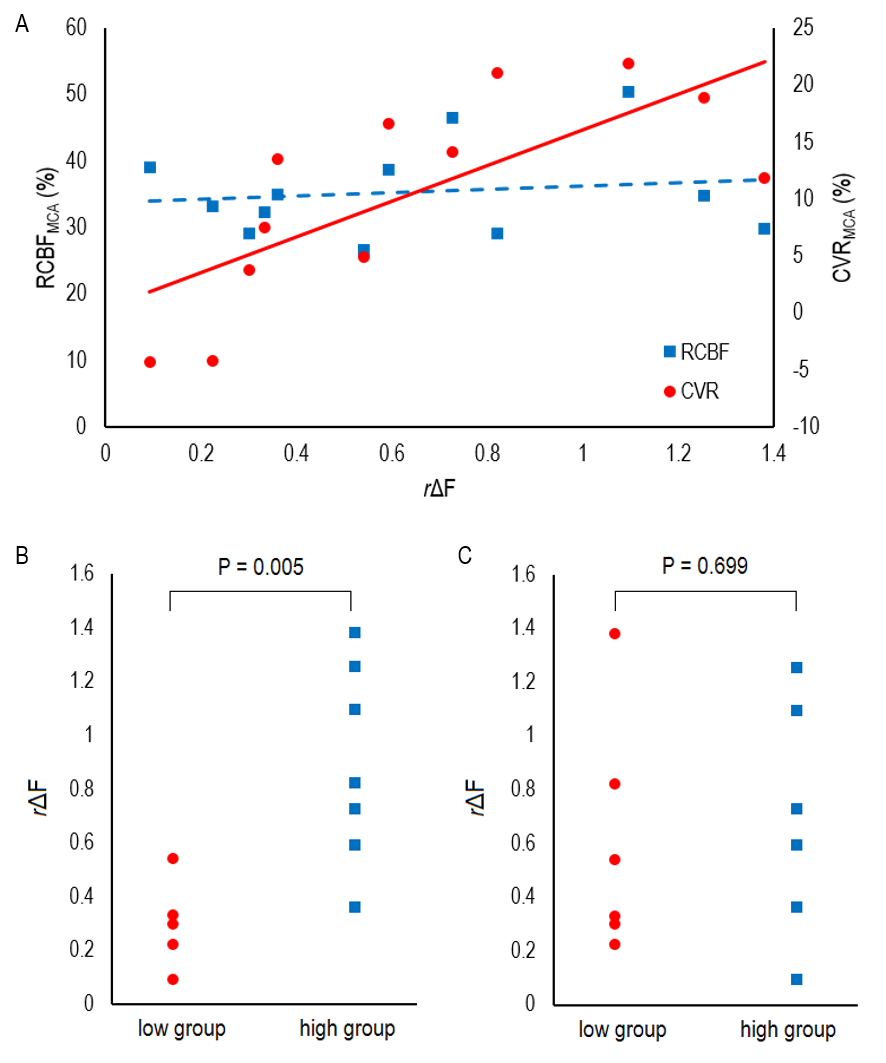
Correlation plots between the rΔF and SPECT data (CVRMCA and RCBFMCA) are shown in Fig. 2A. The correlation between rΔF and CVRMCA were significant (r = 0.800, P = 0.003) while the correlation between rΔF and RCBFMCA were not significant (r = 0.030, P = 0.939). rΔF was significantly lower in the low CVR group than in the high CVR group (0.30±0.16 VS. 0.89±0.37, P=0.008), while there was no significant difference of rΔF between low RCBF group and high RCBF group (0.60±0.44 VS. 0.69±0.44, P=0.739;) (Fig. 2B,2C). Cut-off value of rΔF derived from receiver-operating-curve analysis for misery perfusion based on the values of both CVR and RCBF was 0.592 (Sensitivity 75%, specificity 100% AUC: 0.844) (Fig. 3). Representative cases are shown in Fig. 4 and 5.Discussion
The current study revealed that the ration of pulsatile flow volume of MCA significantly correlates to CVR and identifies misery perfusion with high specificity. We applied the ratio of pulsatile flow volume not pulsatile flow volume of affected side itself. The reason is that the pulsatile flow volume is highly affected by global atherosclerosis, cardiac function and valve diseases which co-exist in patients with atherosclerosis (2). With dividing by pulsatile flow volume of contralateral (normal) side, these effects could be minimized.Conclusion
The ratio of pulsation derived from standard 4D Flow MRI with a 6 min-scan can identify misery perfusion of the patients with ICS.Acknowledgements
This work was supported by JSPS KAKENHI (Grant Number 17K18160), Kurata Grants from the Hitachi Global Foundation (Grant Number 1309) and research grants from Fukuda Foundation for Medical Technology.References
1. Kuroda S, Houkin K, Kamiyama H, Mitsumori K, Iwasaki Y, Abe H. Long-term prognosis of medically treated patients with internal carotid or middle cerebral artery occlusion: can acetazolamide test predict it? Stroke. 2001;32:2110-2116.
2. Michel E, Zernikow B. Gosling's Doppler pulsatility index revisited. Ultrasound Med Biol. 1998;24:597-599.
3. Wahlin A, Ambarki K, Birgander R, et al. Measuring pulsatile flow in cerebral arteries using 4D phase-contrast MR imaging. AJNR Am J Neuroradiol. 2013;34:1740-1745.
4. Sekine T, Amano Y, Takagi R, Matsumura Y, Murai Y, Kumita S. Feasibility of 4D flow MR imaging of the brain with either Cartesian y-z radial sampling or k-t SENSE: comparison with 4D Flow MR imaging using SENSE. Magn Reson Med Sci. 2014;13:15-24.
5. Kataoka H, Miyamoto S, Ogasawara K, et al. Results of Prospective Cohort Study on Symptomatic Cerebrovascular Occlusive Disease Showing Mild Hemodynamic Compromise [Japanese Extracranial-Intracranial Bypass Trial (JET)-2 Study]. Neurol Med Chir (Tokyo). 2015;55:460-468.
Figures