1222
Evaluation of non-contrast enhanced 4-dimensional MRA with stack-of-stars golden angle radial trajectory in conjunction with KWIC reconstruction for the depiction of arteriovenous malformationsLirong Yan1, Songlin Yu2, Samantha Ma1, Jonathan Russin3, Arun Amar3, Yelong Shen1,4, Qi Huang1,5, Nader Pouratian6, Hee Kwon Song7, and Danny JJ Wang1
1Stevens Neuroimaging and Informatics Institute, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 2Beijing Tiantan Hospital, Beijing, China, 3Department of Neurological Surgery, Keck School of Medicine, University of Southern California, Los Angeles, CA, United States, 4School of Medicine, Shandong University, Jinan, China, 5Department of Biomedical Engineering, University of Southern California, Los Angeles, CA, United States, 6Neurosurgery, University of California Los Angeles, Los Angeles, CA, United States, 7University of Pennsylvania, Philadelphia, PA, United States
Synopsis
This study evaluated a recently developed non-contrast enhanced 4-dimensional MRA (NCE 4D MRA) with stack-of-stars golden-angle radial trajectory and KWIC reconstruction for the detection of cerebral arteriovenous malformation (AVM) by comparison with DSA,
Introduction
The evaluation of hemodynamic patterns plays an important role in clinical diagnosis of arteriovenous malformations (AVM). Non-contrast enhanced 4-dimensional MR angiography (4D MRA)1,2 has demonstrated its potential clinical utility in AVM detection3. However, prolonged scan time (6 to 12min) resulting from the multi-phase segmented 3D Cartesian acquisition could hamper its applications. Recently, a 4D MRA with stack-of-stars (SOS) golden-angle radial sampling in conjunction with K-space weighted image contract (KWIC) reconstruction4 has been developed, which can accelerate imaging speed by 3 fold while preserving high spatiotemporal resolution. The aim of this study was to assess the NCE 4D MRA with SOS golden-angle radial acquisition for the characterization of arteriovenous malformation.Methods
All experiments were performed on Siemens Tim Trio and Prisma 3T scanners using product 12- or 20-channel head coil. Eighteen patients who had cerebral AVM underwent NCE 4D MRA scans with Cartesian and SOS radial acquisitions with matched imaging parameters (voxel size: 1.1x1.1x1.5mm3 (Cartesian) and 1x1x1.5mm3 (radial), temporal resolution is approximately 100ms, 25 times frames). 32 slices were acquired leading to a total scan time of approximate 7 and half minutes and 3 minutes for Cartesian and radial samplings, respectively. Variable flip angle scheme (Flip angle: 20-35o)5 was applied during the bSSFP acquisition to improve the delineation of distal arteries in 4D MRA. By taking advantage of rapid acquisition in radial 4D MRA, two image slabs were collected using radial acquisition in some patients to cover the entire lesion. TOF and DSA images were also acquired on patients. Radial data was reconstructed using KWIC method6. Spetzler–Martin grading scale was evaluated with 4D MRA with both Cartesian and radial acquisition, TOF, 4D MRA plus TOF, and DSA respectively by two neuroradiologists. Diagnostic confidence scores for three components of AVMs (feeding artery, nidus and draining vein) were graded from 1 (poor imaging quality with severe artifacts and no diagnostic value) to 5 (excellent imaging quality with no artifacts and definite diagnosis)3. Kendall's coefficient of concordance was calculated to evaluate the reliability between two raters within each modality. A Kendall’s coefficient with higher than 0.75 is considered to indicate excellent agreement. The Wilcoxon signed-rank test was applied to compare the diagnostic confidence scores between each pair of the four techniques for each component of an AVM, respectively.Results
4D MRA images have been successfully obtained from all patients. 16 out of 18 patients had AVM lesions detected by DSA (Table 1). The Spetzler–Martin grading scores in 4D MRA are in complete accordance with those of DSA for feeding artery and nidus, except 4D MRA failed to detect one small lesion (6mm) with low blood flow which was manifested as lightly stained on DSA (Patient #15). 4D MRA is largely consistent with DSA for detecting draining veins in 12/16 cases. Radial 4D MRA performed better than Cartesian (Table 2) in terms of delineation of feeding arteries, nidus and draining veins due to its insensitivity to motion (p<0.01). Figure1 shows 4D MRA images with Cartesian and radial trajectories from an AVM patient. The dynamic filling of labeled blood through feeding arteries, nidus and draining veins is successfully depicted, which matches well with the DSA result. Compared to Cartesian, background tissue signal is markedly suppressed in radial acquisition due to its robustness to motion. Radial acquisition allows doubling imaging volumes under the similar scan time of Cartesian acquisition, offering better delineation of the entire lesion (Figure 2). Relatively high scores of diagnostic confidence were obtained in terms of depiction of feeding arteries and nidus in both radial 4D MRA and TOF, but poor diagnostic confidence was noticed in detection of draining veins. By taking advantage of dynamic flow information in 4D MRA, TOF combined with 4D MRA offers improved diagnostic confidence (p<0.01) (Table2).Discussion and conclusion
This study demonstrates the feasibility of 4D MRA with SOS golden-angle radial sampling and KWIC reconstruction for the evaluation of hemodynamics in cerebrovascular malformations. Compared to Cartesian acquisition, radial 4D MRA shows better performance on characterization of AVM because of robustness to motion. Both TOF and 4D MRA belong to flow-driven technique, resulting in relatively poor depiction of draining veins. Nevertheless, the combination of 4D MRA and TOF can improve overall diagnostic confidence in delineation of AVM lesion. Our findings suggest 4D MRA with SOS golden-angle radial acquisition may become a promising alternative approach for evaluation of AVM due to its markedly reduced scan time and robustness to motion. Noninvasive 4D MRA may reduce the need for DSA and may enhance treatment planning for these complex lesions.Acknowledgements
This work is supported by grants NIH R01EB014922 and AHA16SDG29630013.References
- Yan L, Wang S, Zhuo Y, Wolf RL, Stiefel MF, An J, et al. Unenhanced dynamic mr angiography: High spatial and temporal resolution by using true fisp-based spin tagging with alternating radiofrequency. Radiology. 2010;256:270-279
- Bi X, Weale P, Schmitt P, Zuehlsdorff S, Jerecic R. Non-contrast-enhanced four-dimensional (4D) intracranial MR angiography: a feasibility study. Magn Reson Med. 2010 Mar;63(3):835-41.
- Yu S, Yan L, Yao Y, Wang S, Yang M, Wang B, et al. Noncontrast dynamic mra in intracranial arteriovenous malformation (avm), comparison with time of flight (tof) and digital subtraction angiography (dsa). Magnetic resonance imaging. 2012;30:869-877
- Song HK, Yan L, Smith RX, Xue Y, Rapacchi S, Srinivasan S, at al. Noncontrast enhanced four-dimensional dynamic MRA with golden angle radial acquisition and K-space weighted image contrast (KWIC) reconstruction. Magn Reson Med. 2014 Dec;72(6):1541-51.
- Schmitt P SP, Bi X, Weale P, Mueller E. Non-contrast-enhanced 4d intracranial mr angiography: Optimizations using a variable flip angle approach. Proceedings of the Eighteenth Meeting of the International Society for Magnetic Resonance in Medicine. 2011.
- Song HK, Dougherty L. k-space weighted image contrast (KWIC) for contrast manipulation in projection reconstruction MRI. Magn Reson Med. 2000;44:825–832.
Figures
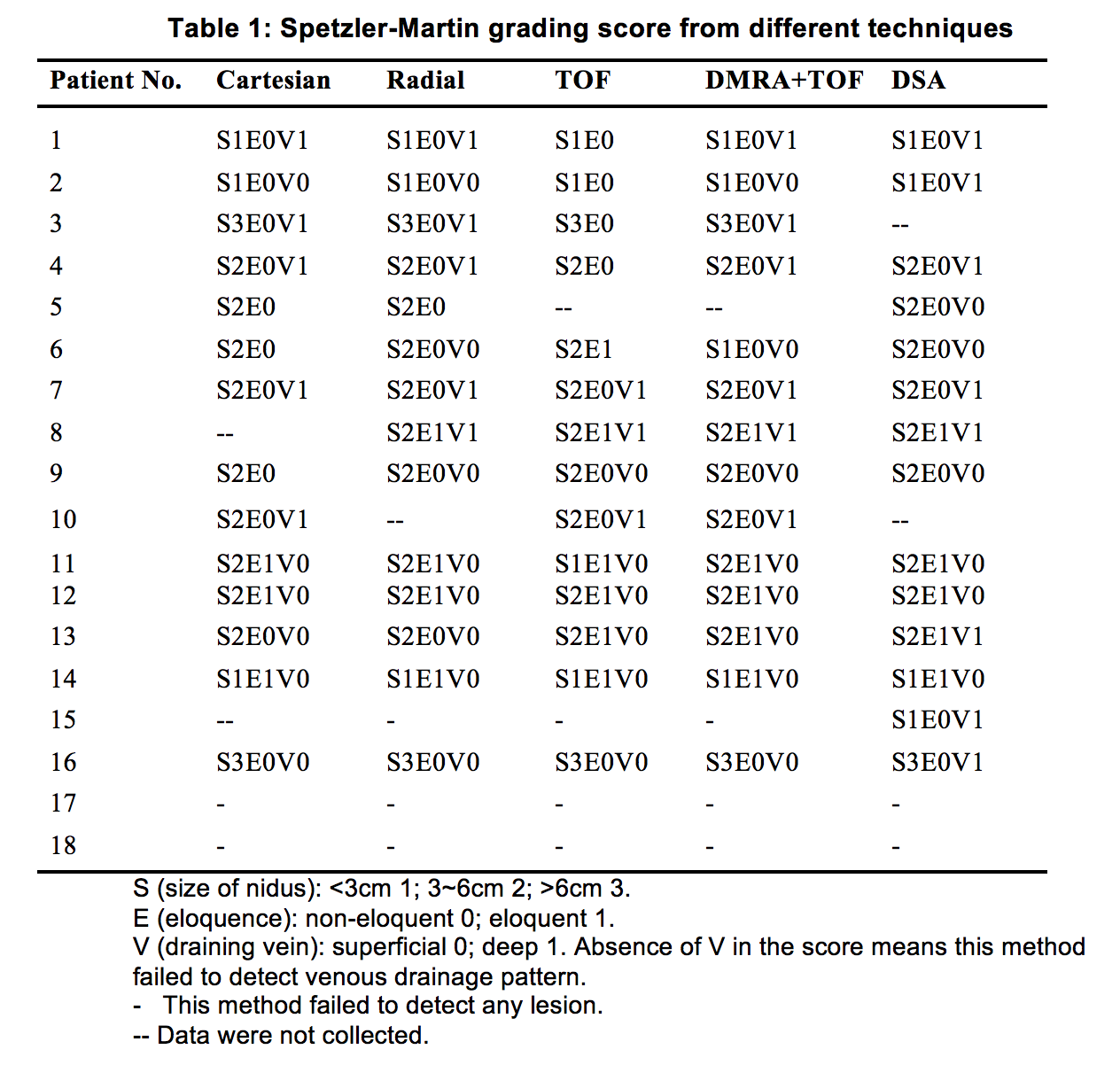
Table 1. Spetzler-Martin grading score from different techniques
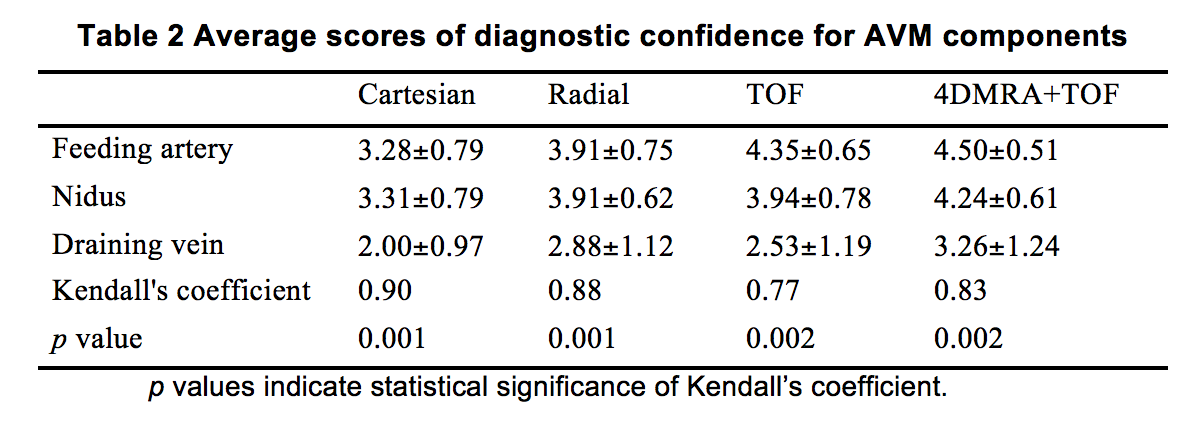
Table 2
Average scores of diagnostic confidence for AVM components
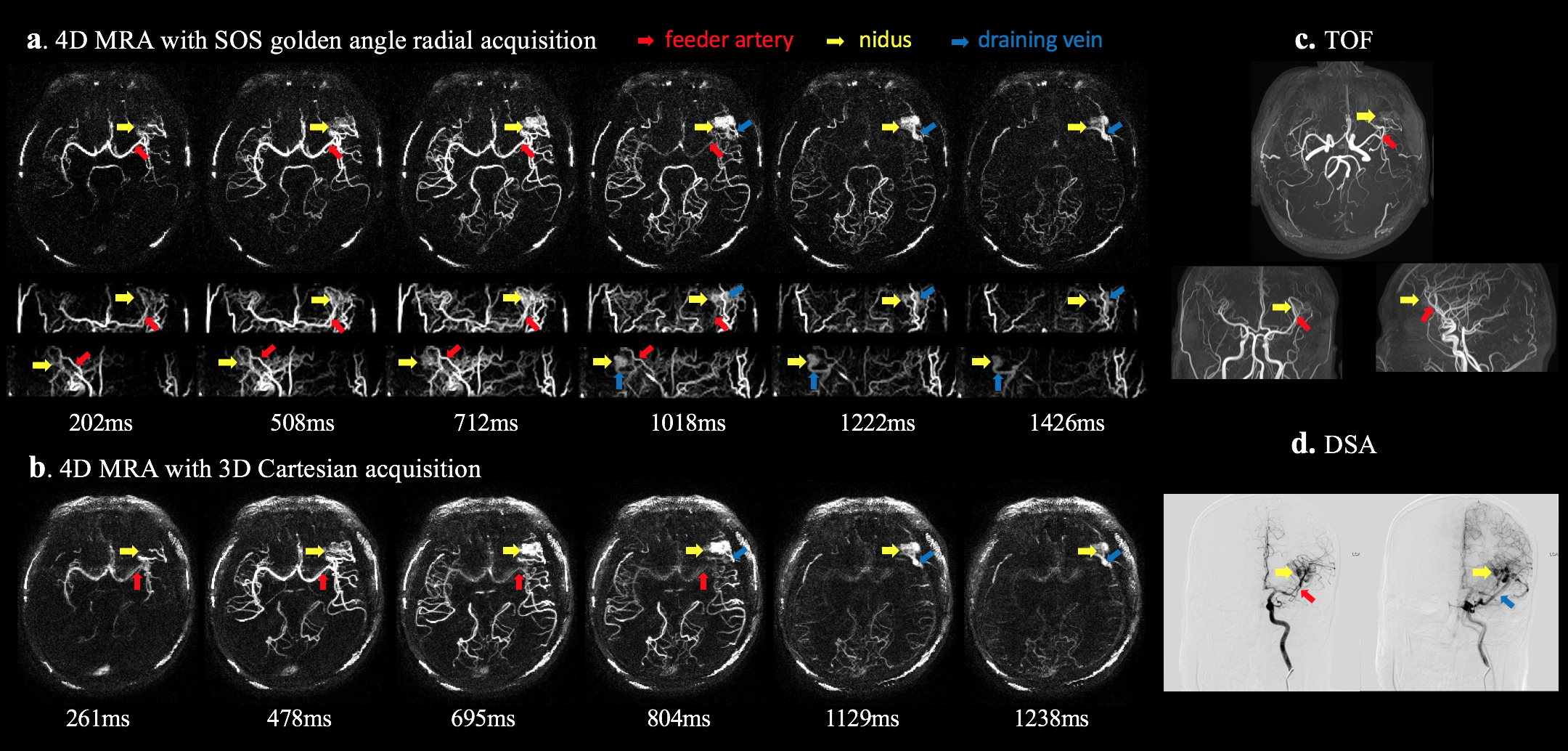
Figure 1. Patient who had left frontotemporal AVM underwent craniotomy surgery. Follow-up imaging was performed 3 years later. From 4D MRA images, we can clearly visualize the dynamic filling of labeled blood from feeding arteries (MCA, red arrows), through abnormal vascular nidus (yellow arrow) and then into the draining views (blue arrow) sequentially which was in accordance with findings of DSA. However, TOF only detected the nidus faintly and failed to detect draining vein.
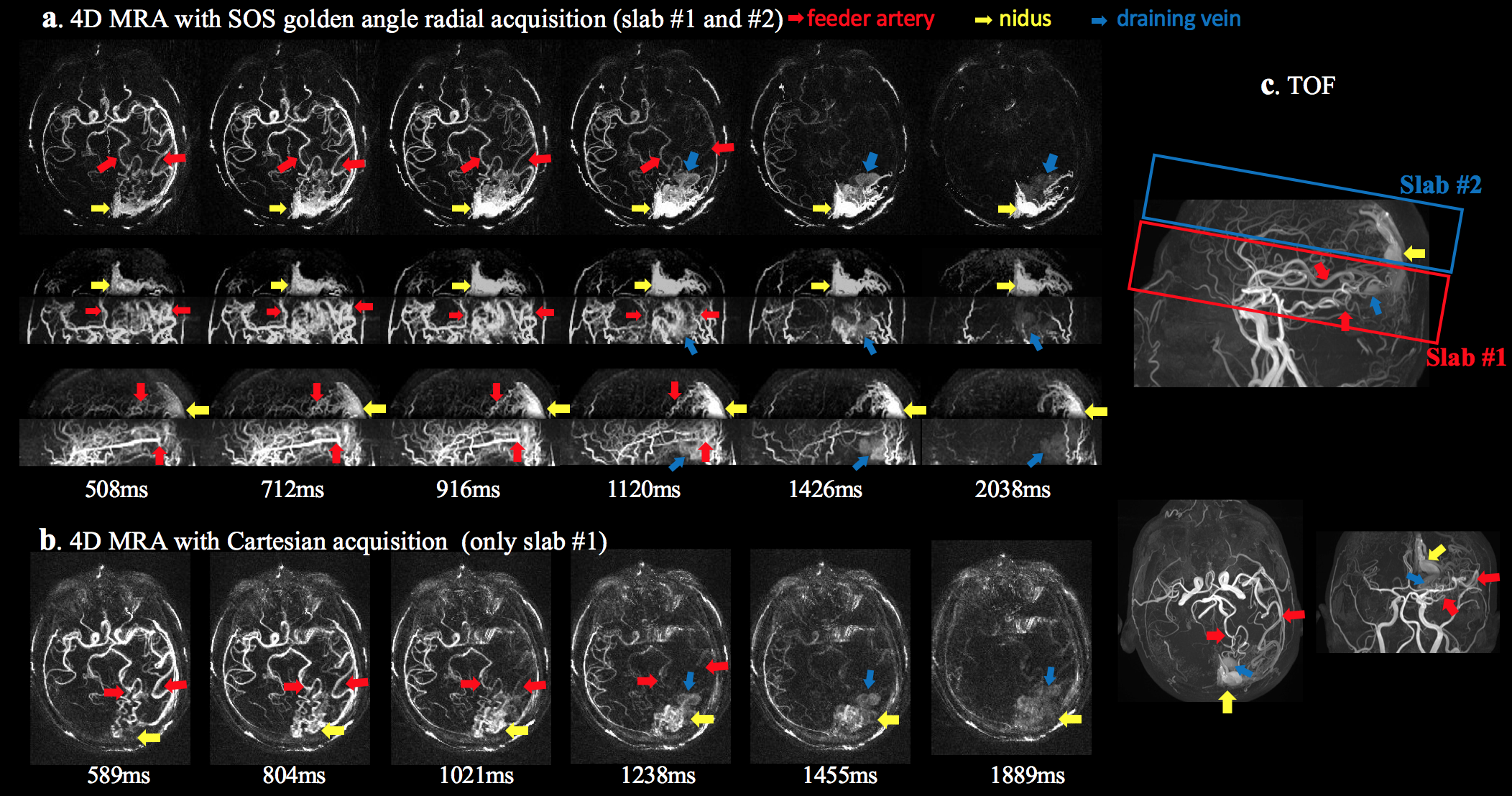
Figure 2. Patient with AVM lesion in left occipital lobe. To fully cover the lesion, two slabs were acquired using 4D MRA with radial acquisition leading to a scan time of approximate 6mins. Compared to single-slab Cartesian images (7.5mins), one can clearly observe the dynamic course for labeled blood from feeding arteries (MCA and PCA, red arrow), through entire nidus (yellow arrow) and then into the draining veins (blue arrow) sequentially.