1180
Texture analysis of multiparametric MRI in cervical cancer before and after chemoradiotherapy1Diagnostic Radiology, The University of Hong Kong, Hong Kong, Hong Kong, 2Philips Healthcare, Hong Kong, Hong Kong
Synopsis
Texture analysis of multiparametric MRI (mpMRI) consisting of diffusion-weighted MRI (DWI) and T2-weighted (T2W) texture features could be a promising quantitative approach in assessing tumor heterogeneity. We retrospectively studied forty patients who had paired mpMRI examinations before and at week-4 of chemoradiotherapy (CRT). Based on the changes in stable mpMRI features, we observed that initially more anatomically and functionally homogenous tumors had better response to treatment and that tumors became more functionally heterogenous after treatment.
Purpose
To evaluate the ability of texture analysis to quantify tumor heterogeneity and its association with treatment response.Methods
Forty patients with treatment-naïve cervical cancer who underwent whole-pelvis CRT were retrospectively analyzed. Two sequential MRI examinations were performed on a 3.0T TX Achieva scanner (Philips Healthcare) at pre-treatment (MRI1) and week-4 of CRT (MRI2).
DWI was acquired suing single-shot spin echo echo-planar imaging in free breathing (b = 0-1,000 s/mm2). Conventional T2W sequences were also acquired. Two radiologists independently delineated volumetric regions of interest (VOIs) to encompass the whole cervical tumor.
Images were normalized by applying a µ±3σ threshold and then discretized into 64 gray levels1. Four families of mpMRI features (Table 1) were extracted, totaling 100 features. For direction-dependent features, directions were averaged for rotational invariance. For features that depend on the distance of measurements, fine, medium, and coarse variants were extracted.
To assess interobserver variability of texture features, and to preform feature reduction, Bland-Altman analysis was used. Acceptable interobserver variability was defined as having a limits of agreement (LoA) of less than 10% which was calculated by:
$$$LoA = \bar{d} \pm 1.96s$$$
Where $$$\bar{d}$$$ is the mean difference between measurements and s is the standard deviation of those differences2. Only features with acceptable interobserver variability was used in subsequent analysis
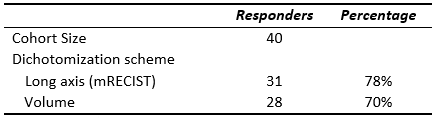
The longest axes of tumors, and primary tumor volume (PTV) was evaluated on T2W. Response to CRT was dichotomized into responder and non-responder groups by two schemes: 20% longest axes reduction3 and 65% volumetric reduction4 were considered as responders in the first and second schemes respectively.
The Mann-Whitney U test was first used to determine significantly different mpMRI features at MRI1 between responders and non-responders. The final value at MRI2 of these significantly different features was also compared between responders and non-responders. The paired t-test was used in sub-group analysis to evaluate the change mpMRI features over the course of treatment dichotomized by response groups.
Results
Texture features with acceptable interobserver variability are marked in Table 1. Response dichotomization was summarized in Table 2. At MRI1, there was no significant difference in PTV between response groups, but at MRI2, responders had significantly smaller tumors (Table 3).
When using the axis dichotomization scheme, there were no significant differences in mpMRI features between responders and non-responders at MRI1.
When using the volumetric dichotomization scheme: a mixture of DWI and T2W features from both Gray Level Co-Occurence Matrix (GLCM) and Gray Level Run Length Matrix (GLRLM) families were significantly different between responders and non-responders at MRI1. Of these features, only T2W Short Run High Gray Level Emphasis (SRHGLE) remained significantly different at MRI2. Results of significant mpMRI features at both timepoints are tabulated on Table 3.
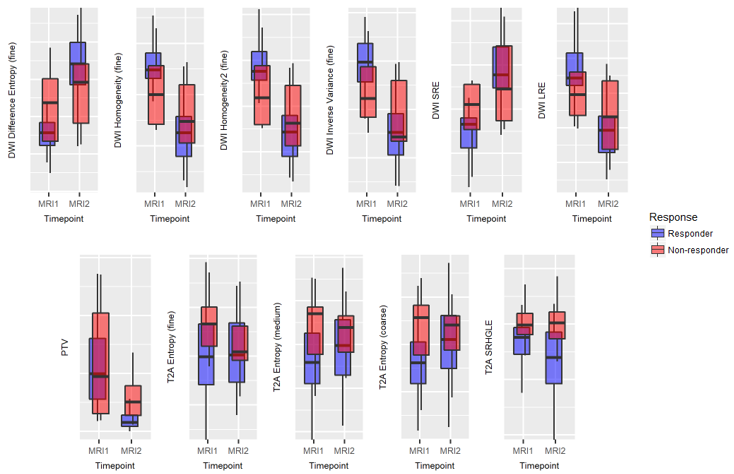
In sub-group analysis, over the course of treatment, all DWI features were significantly different between MRI1 and MRI2 in both responders and non-responders. Furthermore, all DWI features trended towards higher heterogeneity. T2W SRHGLE demonstrated a significant decrease in the responder group following treatment, but did not demonstrate a corresponding decrease in the non-responder group. Results of the changes in significant mpMRI features are visualized in Figure 1.
Discussion
In our study, response groups could not be separated by baseline PTV, suggesting that tumor heterogeneity critically influence treatment outcome5,6. Quantification of the spatial heterogeneity of cervical cancer has been shown to be useful in predicting treatment response7,8 with texture analysis becoming the preferred methodology of heterogeneity assessment9.
The current method of assessing treatment response is the modified Response Evaluation Criteria in Solid Tumors (mRECIST). However, since the method dichotomizes patients based on a single dimension, it maybe not as reliable in tumors that respond in a heterogenous fashion10. One study suggested that volumetric criterion replace the axial criterion4, especially if texture features are extracted on tumor volumes.
At baseline, we observed that tumors with higher baseline DWI and T2W homogeneity have better prognosis and had better response.
Over the course of treatment, DWI features trended to higher heterogeneity, and after treatment, there were no significant differences in DWI features between the two response groups. This was in concordance with a previous histogram analysis study11 which suggests that responders and non-responders have similar diffusivity profiles after treatment.
Of the significantly different textures between response groups at baseline, only T2W SRHGLE remained different at the end of CRT. This suggests that tumors with good response are characterized as anatomically homogeneous residual tumors following treatment compared to tumors with poor response.
Conclusion
Texture analysis of mpMRI is a potentially useful technique in quantifying the spatial differences in anatomical and diffusion profiles of cervical cancer before and after CRT.Acknowledgements
No acknowledgement found.References
1. Collewet, G., Strzelecki, M. & Mariette, F. Influence of MRI acquisition protocols and image intensity normalization methods on texture classification. Magnetic Resonance Imaging 22, 81-91 (2004). 2. Bland, J.M. & Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. The lancet 327, 307-310 (1986).
3. Lencioni, R. & Llovet, J.M. Modified RECIST (mRECIST) assessment for hepatocellular carcinoma. in Seminars in liver disease, Vol. 30 052-060 (© Thieme Medical Publishers, 2010).
4. Lin, M., Pellerin, O., Bhagat, N., Rao, P.P., Loffroy, R., Ardon, R., Mory, B., Reyes, D.K. & Geschwind, J.-F. Quantitative and Volumetric EASL and RECIST: Feasibility of a Semi-automated Software Method to Assess Tumor Response after Transcatheter Arterial Chemoembolization (TACE). Journal of vascular and interventional radiology : JVIR 23, 1629-1637 (2012).
5. Mayr, N.A., Huang, Z., Wang, J.Z., Lo, S.S., Fan, J.M., Grecula, J.C., Sammet, S., Sammet, C.L., Jia, G., Zhang, J., Knopp, M.V. & Yuh, W.T. Characterizing tumor heterogeneity with functional imaging and quantifying high-risk tumor volume for early prediction of treatment outcome: cervical cancer as a model. Int J Radiat Oncol Biol Phys 83, 972-979 (2012).
6. Marusyk, A., Almendro, V. & Polyak, K. Intra-tumour heterogeneity: a looking glass for cancer? Nature reviews. Cancer 12, 323 (2012).
7. Mayr, N.A., Yuh, W.T., Arnholt, J.C., Ehrhardt, J.C., Sorosky, J.I., Magnotta, V.A., Berbaum, K.S., Zhen, W., Paulino, A.C. & Oberley, L.W. Pixel analysis of MR perfusion imaging in predicting radiation therapy outcome in cervical cancer. Journal of Magnetic Resonance Imaging 12, 1027-1033 (2000). 8. Torheim, T., Malinen, E., Kvaal, K., Lyng, H., Indahl, U.G., Andersen, E.K. & Futsaether, C.M. Classification of dynamic contrast enhanced MR images of cervical cancers using texture analysis and support vector machines. IEEE Transactions on medical imaging 33, 1648-1656 (2014).
9. Chicklore, S., Goh, V., Siddique, M., Roy, A., Marsden, P.K. & Cook, G.J.R. Quantifying tumour heterogeneity in 18F-FDG PET/CT imaging by texture analysis. European Journal of Nuclear Medicine and Molecular Imaging 40, 133-140 (2013).
10. Seyal, A.R., Gonzalez‐Guindalini, F.D., Arslanoglu, A., Harmath, C.B., Lewandowski, R.J., Salem, R. & Yaghmai, V. Reproducibility of mRECIST in assessing response to transarterial radioembolization therapy in hepatocellular carcinoma. Hepatology 62, 1111-1121 (2015).
11. PERUCHO, J., Lee, E., Chan, W., Gong, N. & Chan, Q. Histogram analysis of intravoxel incoherent motion MRI in predicting chemoradiotherapy response in cervical cancer. in The 25th Annual Meeting of ISMRM, Honolulu, Hawaii, USA. 2017 (2017).
Figures
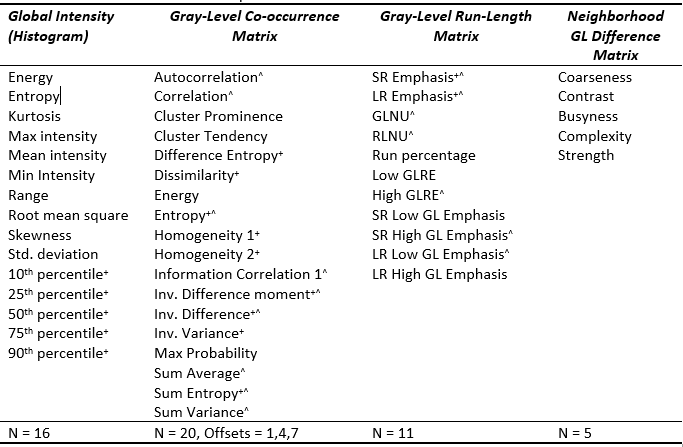
Table 1 Texture features planned for use in this study. Inv.: Inverse; SR: Short run; LR: Long run; GL: Gray-level; Non-Uniformity; RL: Run-Length; RE: Run-Emphasis
+ - DWI texture features that have acceptable interobserver variability
^ - T2W texture features that have acceptable interobserver variability