1142
2D phase contrast MRI to quantify CSF dynamics change after surgery of Chiari “malformations"1imaging processing, university hospital, Amiens, France, 2neurosurgery, university hospital, Amiens, France, 3radiology, university hospital, Amiens, France
Synopsis
Diagnosis of Chiari malformation (CM) is mainly based on morphological. The objective of this study was to quantify the evolution of CSF and blood flows dynamics before and after surgery treatment of CM. 21 patients who underwent surgery for CM, and presented good clinical outcome at 12 months were retrospectively included. We have shown that in CM, CSF flow is mainly reduced at the foramen magnum whereas it is normal at the cervical level. CM reduces jugular outflow. Complementary to the morphological investigation 2D PCMRI should be take in account to improve the evaluation of the severity of the Chiari Malformation.
Introduction
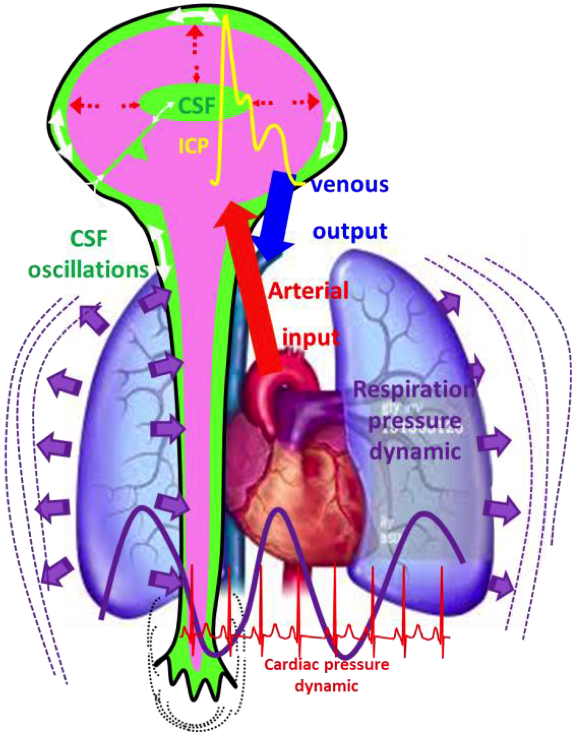
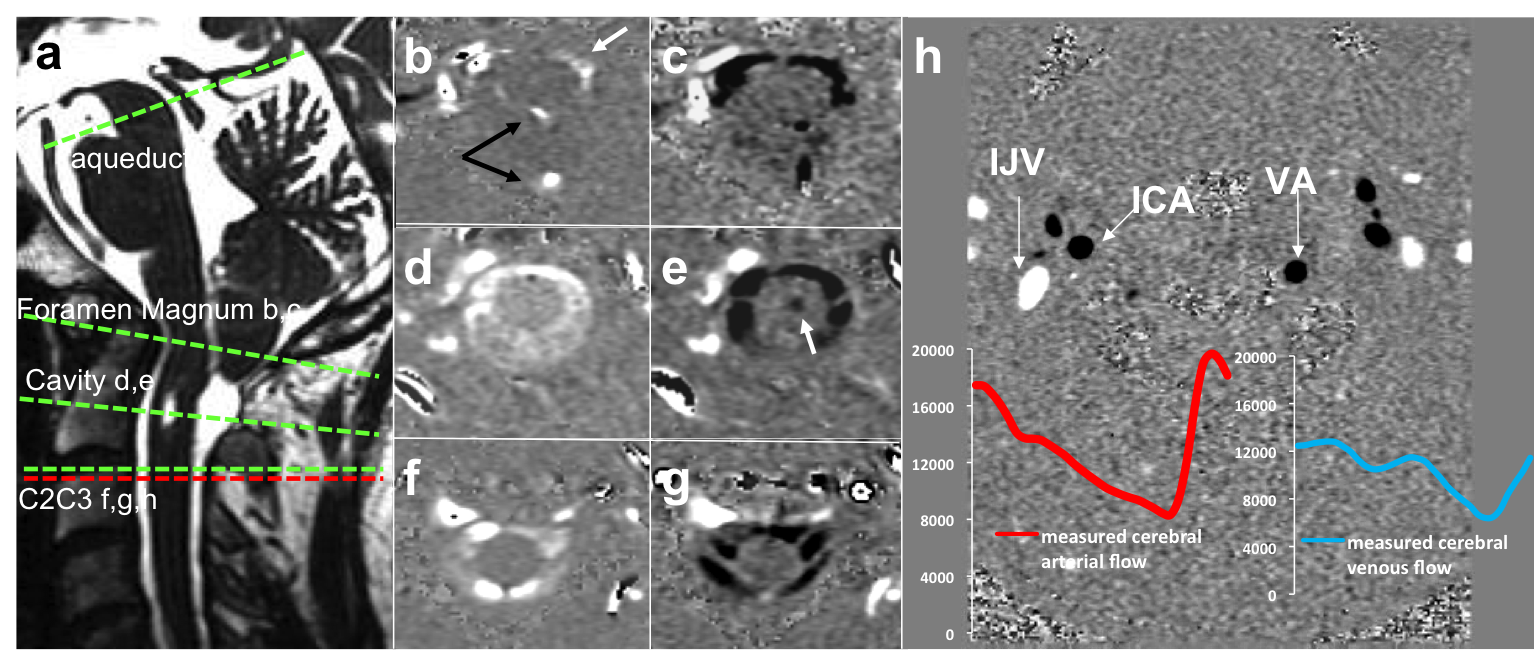
The CSF oscillations provide a part of the compliance of the cranio spinal system during each systolic cerebral vascular expansion in the rigid cranial box (1). Intracranial CSF volume change through the spinal canal avoids large intracranial pressure amplitude during systole (Figure 1). Chiari malformation (CM) consists of a downward displacement of the cerebellar tonsils through the foramen magnum (1) (Figure 2). In some CM people, there may be no associated symptoms, and no intervention is necessary but in others it can become a progressive disorder and lead to serious complications as syringomyelia, hydrocephalus, Tethered cord syndrome or spina bifida. Surgery is the treatment of CM, it involves posterior fossa decompression. Diagnosis of CM is mainly based on morphological images (2-6). PCMRI is the unique tool able to evaluate CSF oscillations (1,4-6). The objective of this study was to quantify the evolution of CSF and blood flows dynamics before and after treatment of Chiari malformation to show if PC-MRI could be helpful in the diagnosis and the follow up outcome of CM patients.Methods
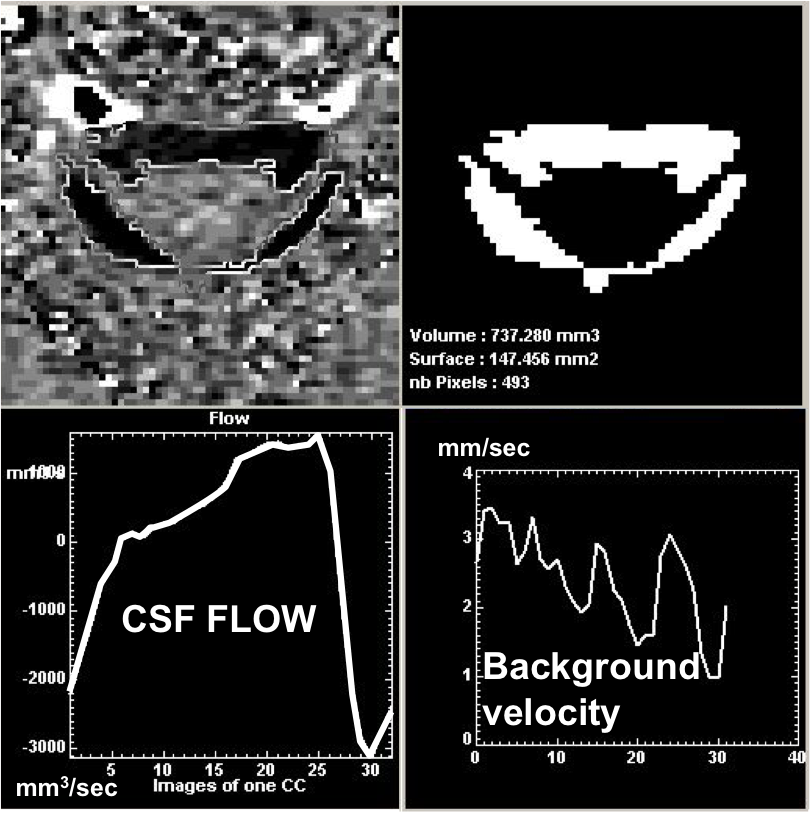
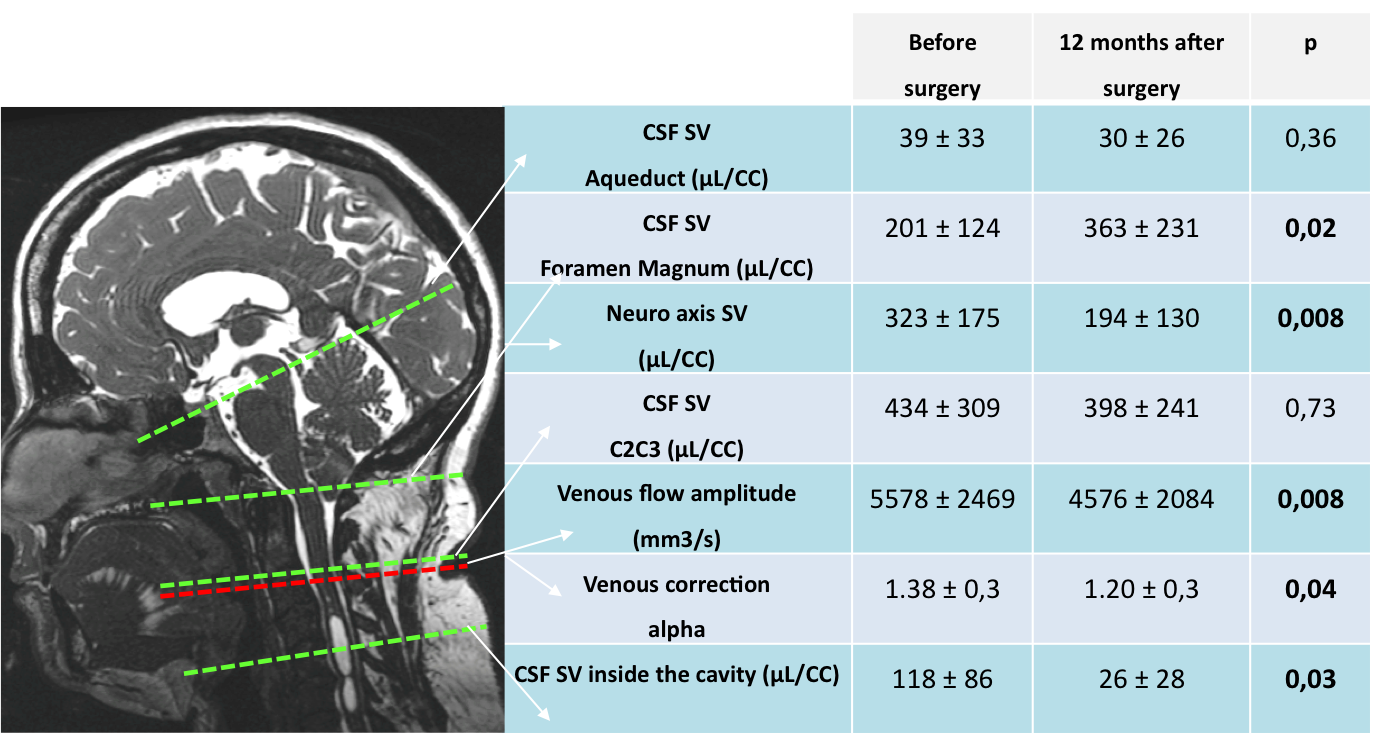
In respect with the ethical law, 21 patients who underwent surgery for Chiari malformation, and presented good clinical outcome at 12 months were retrospectively included. 12 presented a Syringomyelia cavity. Two surgical procedures were applied: occipital bone craniectomy and C1 laminectomy (9 patients), or bone decompression associated with duraplasty (12 patients). Each patient underwent a 3T MRI with phase-contrast sequences during the preoperative evaluation to evaluate CSF and blood flow oscillations. The same MR-scan was performed one year after surgery. PC MRI parameters were: TR and TE minimum; FOV=140 * 140 mm2; 256 mm2 matrix; 5 mm slice thickness; 2 views per segment. Cardiac Synchronization was realized with peripheral gating. Velocity encoding was set to 80 cm/sec for blood and 5-10 cm/sec for CSF. The slice acquisition planes were positioned at different levels perpendicular to the direction of flow (Figure 2). Semi-automatic flow measurements were performed using a dedicated CSF algorithm segmentation (1) to allow rapid accurate and reproducible extraction of the complex anatomy of the CSF areas (Figure 3). The volume displaced during the cardiac cycle or stroke volumes (SV) were calculated for the CSF through : the aqueduct, the arachnoids spaces at the C2C3 level and in the foramen magnum, at this level SV was also calculated for the neuroaxis. Cerebral arterial inflow was calculated by summation of the internal carotids and vertebrals arteries flows. Jugular blood flows were summed. An alpha factor was calculated as the ratio of the global arterial input flows and the jugular flows (1). The amplitude of the flow (maximum-minimum) of the venous outflow was calculated. Comparisons of these parameters before and after surgery were evaluated by a Wilcoxon signed-rank paired testResults
The CSF oscillations, cerebral arterial and juguglar blood flows were easily calculated in all the patients. We show in the figure 4 how the surgery impact or not the CSF and blood flow dynamics. We have found that presence of a syringomyela cavity didn’t affect the values of the different parameters, excepted for the Alpha (arterio venous ratio) parameter which was significantly higher in the Syringomyelia population (1.49±0.4 versus 1.19±0.1;P<0.05)Discussion
PCMRI is an interesting tool, which can easily show and quantitatively evaluate the functional impact of CM in the CSF and blood flows oscillations. In our population CM don’t impact CSF oscillations in the ventricles and at the C2C3 cervical level, but largely impact the CSF circulation at the foramen magnum, which result in a significant movement of the neuroaxis, normally static in healthy population. In fact we think that even if CSF is blocked at the foramen Magnum, movement of the cerebrellar tonsil and the neuroaxis transmit directly transmit the movement to the CSF at the cervical level. This result shows that C2C3 is not a good level to evaluate CM impact in the CSF oscillations. It is also interesting to note that CM reduced the jugular mean outflows and paradoxaly in the same time increased the amplitude of the venous flow. These venous alterations were reversibles and presented good outcome after surgery.Conclusion
Simple 2D PCMRI can evaluate in 10 minutes the impact of CM in the CSF and cerebral blood flow. In CM, CSF flow is mainly reduced at the foramen magnum whereas it is normal at the cervical level. CM reduces jugular outflow. Surgery decompression has a positive impact of the CSF and blood flow circulation. PCMRI appears to be useful to evaluate the surgery procedure outcome and its follow up. Complementary to the morphological investigation 2D PCMRI should be take in account to improve the evaluation of the severity of the Chiari Malformation.Acknowledgements
We thank the MRI technicians for their important help in the acquisitions of all these strange images !We thank the hospital, it trusts and support our researchs.finaly we thanks the Région Picardie for his financial support
References
1 Balédent O, Henry-Feugeas MC, Idy-Peretti I. Cerebrospinal fluid dynamics and relation with blood flow: a magnetic resonance study with semiautomated cerebrospinal fluid segmentation. Invest Radiol. 2001 Jul;36(7):368-77.
2 Koehler PJ. Chiari's description of cerebellar ectopy (1891). With a summary of Cleland's and Arnold's contributions and some early observations on neural-tube defects. J Neurosurg. 1991 Nov;75(5):823-6
3 Milhorat TH1, Nishikawa M, Kula RW, Dlugacz YD. Acta Neurochir (Wien). 2010 Jul;152(7):1117-27. Mechanisms of cerebellar tonsil herniation in patients with Chiari malformations as guide to clinical management.
4 Radmanesh A, Greenberg JK, Chatterjee A, Smyth MD, Limbrick DD Jr, Sharma A. Tonsillar pulsatility before and after surgical decompression for children with Chiari malformation type 1: an application for true fast imaging with steady state precession. Neuroradiology. 2015 Apr;57(4):387-93.
5 Alperin N, Sivaramakrishnan A, Lichtor T. Magnetic resonance imaging-based measurements of cerebrospinal fluid and blood flow as indicators of intracranial compliance in patients with Chiari malformation. J Neurosurg. 2005 Jul;103(1):46-52.
6 Leung V, Magnussen JS, Stoodley MA, Bilston LE. Cerebellar and hindbrain motion in Chiari malformation with and without syringomyelia. J Neurosurg Spine. 2016 Apr;24(4):546-55.
Figures