1048
Single Breath-held, ECG-Free Cardiac CINE MRI using Parallel Imaging and Deep Learning Combined Image Reconstruction1Radiology, University of California, Los Angeles, Los Angeles, CA, United States, 2Radiation Oncology, University of California, Los Angeles, Los Angeles, CA, United States
Synopsis
Cardiac CINE MRI is widely used for evaluating ventricular wall motion and cardiac function. Conventional cardiac CINE consists of ECG-triggered k-space segmented 2D acquisitions, each performed within a breath-hold. In this study, we propose an ECG-free, cardiac CINE protocol that covers the entire LV within a single breath-hold. Our solution is based on a highly accelerated real-time imaging that is enabled by our recently proposed parallel imaging and deep learning combined (PI-DL) image reconstruction. In this study, we evaluated the proposed solution in healthy volunteers and compare its performance with cardiac CINE images acquired using conventional protocol.
Introduction
Cardiac CINE MRI is widely used for evaluating ventricular wall motion and calculating left ventricle (LV) ejection fraction (EF), an important biomarker for cardiac function. Conventional cardiac CINE consists of multiple 2D ECG-triggered segmented acquisitions, each performed within a breath-hold, to cover the entire LV[1]. However, the ECG signal often has reliability issues due to interferences with the magnetic field. In addition, the repeated breath-holds not only increase the time and complexity of the exam, but also introduce additional measurement errors due to slice miss-registration among breath-holds. To address these issues, we propose an ECG-free, cardiac CINE protocol that covers the entire LV within a single breath-hold. Our solution is based on a highly accelerated real-time imaging that is enabled by our recently proposed parallel imaging and deep learning combined (PI-DL) image reconstruction. In this study, we evaluated the proposed solution in healthy volunteers and compare its performance with cardiac CINE images acquired using conventional protocol.Methods
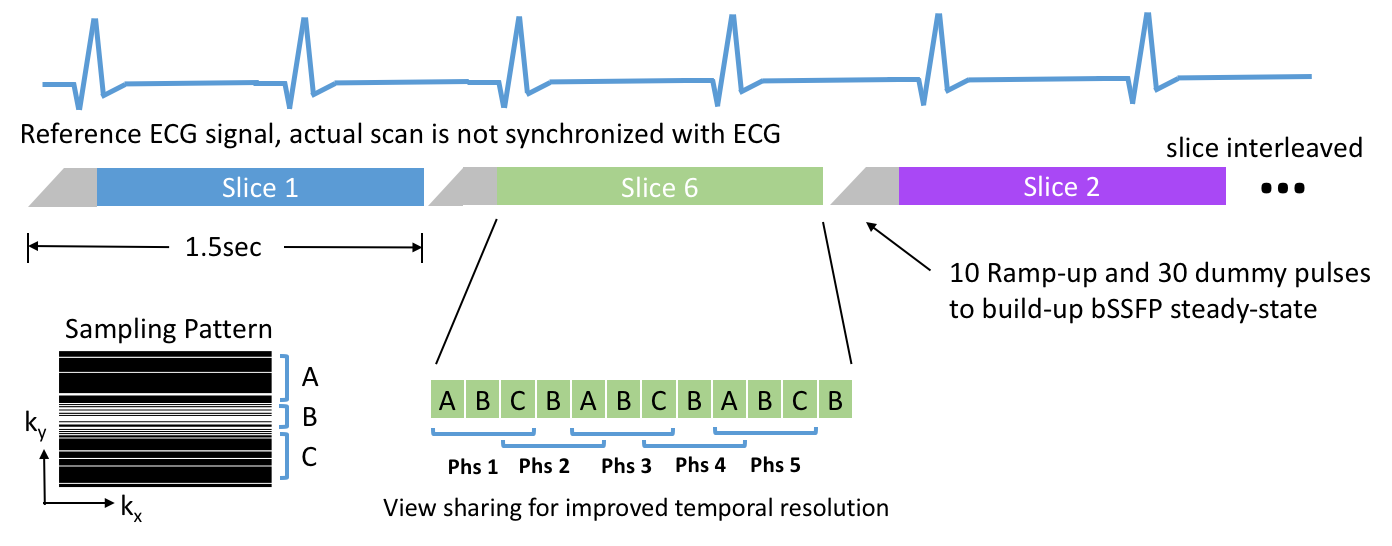
Our protocol (Fig.1) is based on highly accelerated real-time sequence, the 2D k-space was under-sampled 5X using variable density sampling to achieve 72ms temporal resolution. View-sharing was used to further reduce the temporal resolution to 48ms. Images were acquired in real-time without ECG-triggering and k-space segmentation. The acquisition of 10 short-axis slices was performed in a slice-interleaved fashion and each slice was scanned for 1.5 seconds to ensure complete coverage of an entire cardiac cycle. The protocol takes 15 seconds and was fitted into a single breath-hold.
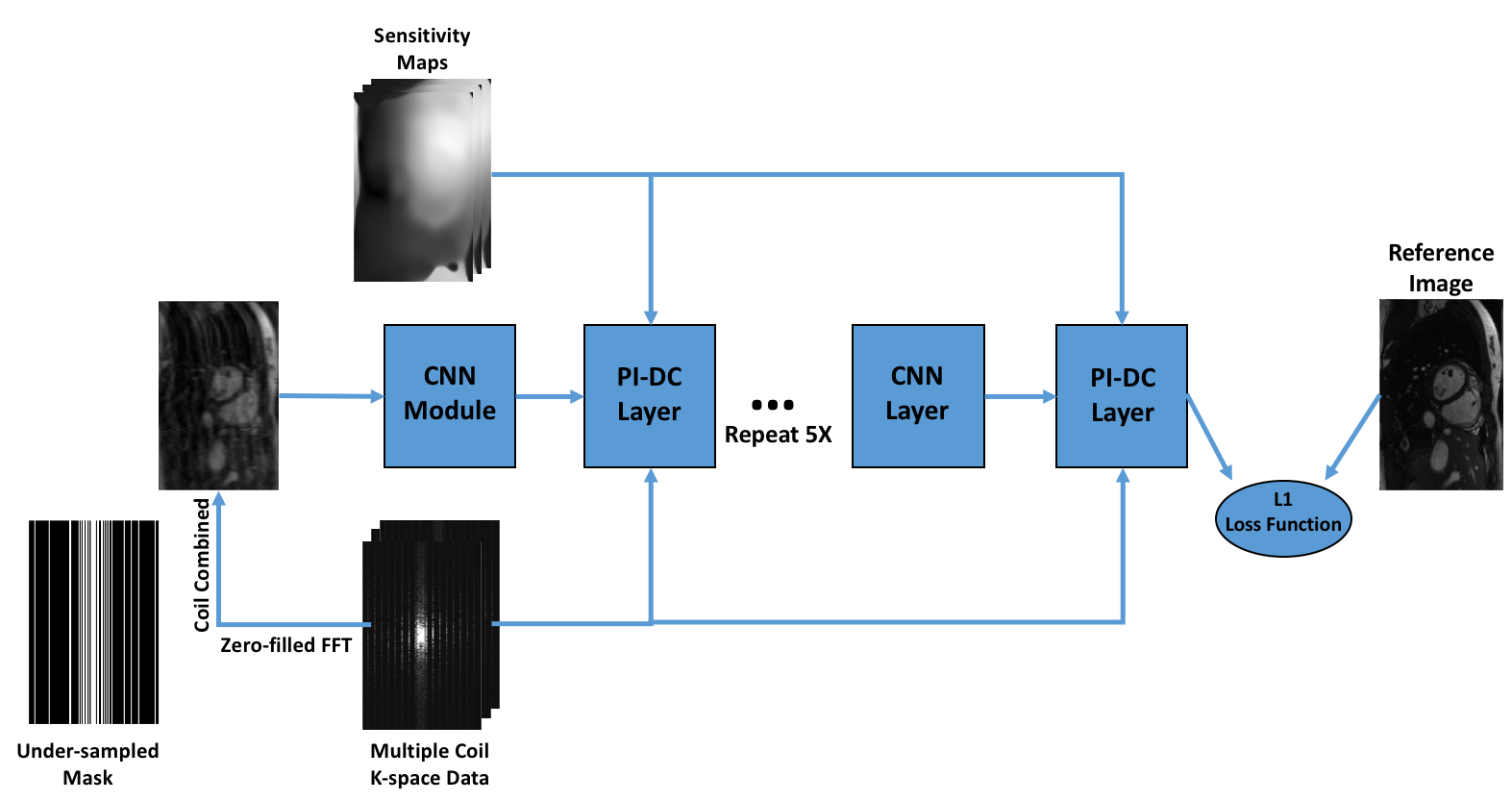
The images were reconstructed using our recently proposed PI-DL method (Fig.2). The algorithm maps the zero-filled, coil-combined images to fully sampled ones using a multi-layer convolutional neural network (CNN) [2-3]. Multiple parallel imaging data consistency (PI-DC) layers were inserted into the CNN to utilize the coil sensitivity information and multi-coil k-space data for improved performance. The coil sensitivity maps used in this study were estimated from center k-space lines using the ESPIRiT algorithms [4]. The details of the PI-DL algorithm are described in a separate submission.
Our study includes 7 healthy volunteers. Conventional cardiac CINE protocol was performed on all subjects, with the following parameters: (TE/TR=1.2/2.8ms, flip angle=60º, matrix=192x120, slice thickness=8mm, 10 slices in 10 breath-holds, resolution=1.5-1.6mm2, 20-25 phases). The fully sampled k-space from conventional CINE was retrospectively under-sampled to form the training dataset, which consists of 1200 training samples from the first 5 subjects. This dataset was randomized and divided into training (800 samples), validation (200 samples) and testing (200 samples) datasets. The proposed ECG-free single breath-held CINE protocol was performed on the 6th and 7th subjects. The matrix size and spatial resolution were identical to the conventional CINE protocol. Other important sequence parameters include: (temporal resolution: 48ms (view sharing), 15s single breath-hold, no ECG triggering). Real-time cardiac CINE images were reconstructed from under-sampled k-space using the trained CNN network. The ECG-free single breath-hold cardiac CINE images were compared with the ones from the conventional protocol. LV was manually contoured by an MR physicist and the blood-pool area of each slice/phase were calculated and compared between the images from two protocols.
Results
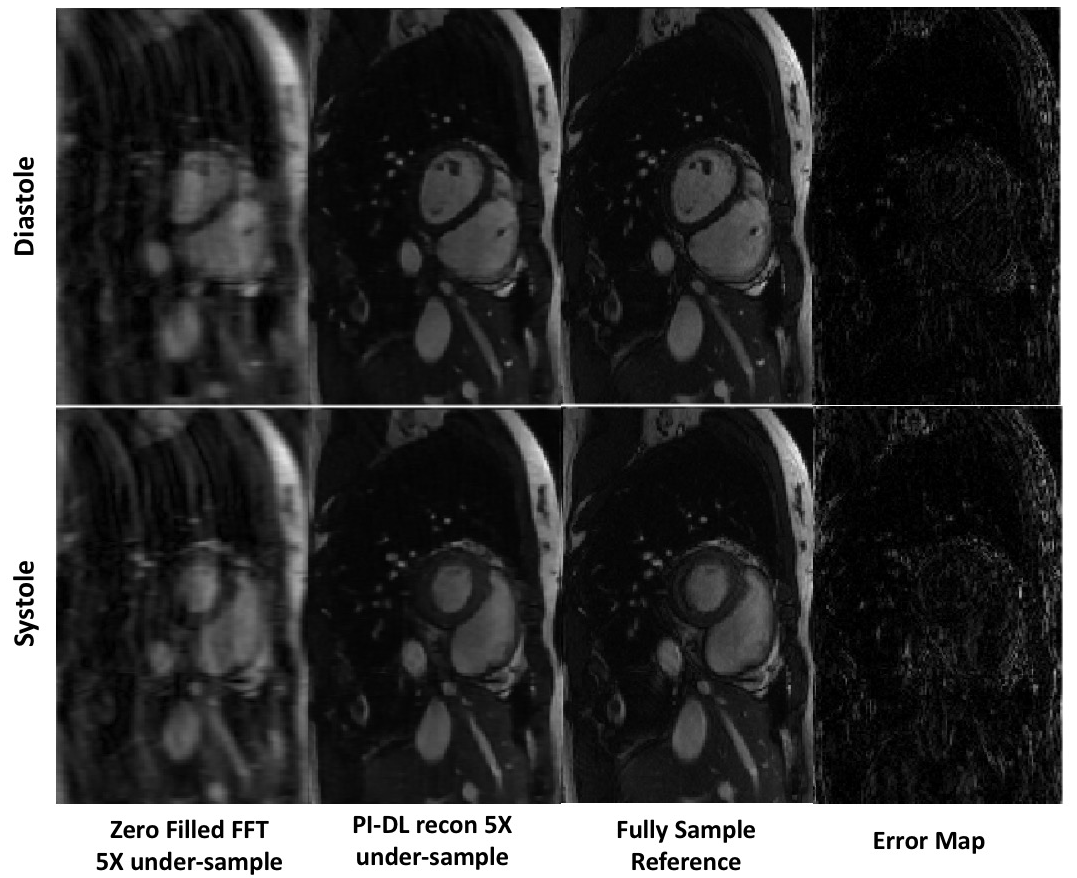
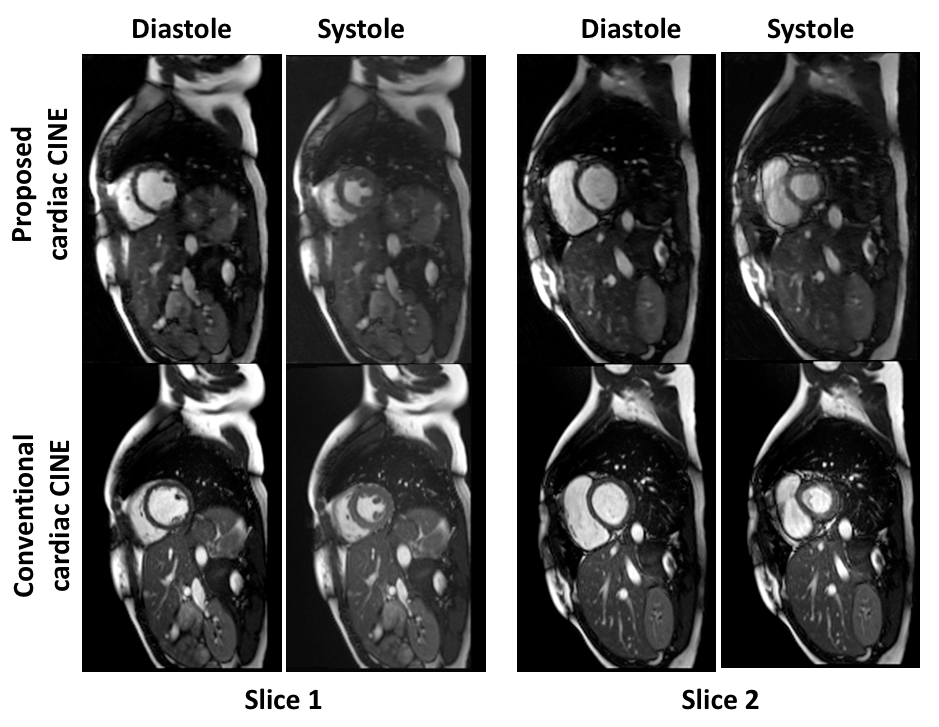
The training of the CNN takes 12 hours on a Linux workstation (Intel i7 3.9GHz, 64GB RAM, Nvidia GTX780 GPU). The reconstruction of each prospectively under-sampled k-space took 40ms using the trained network. Fig.3 shows the comparison of images reconstructed from zero-filled k-space, proposed PI-DL algorithms and reference. The averaged normalized root mean square error (nRMSE) between the PI-DL and the reference images in the testing dataset was 0.354, although the systole phases tend to have slightly errors than the diastole phases, as demonstrated in the error maps in Fig.3. Fig.4 shows the cardiac CINE images using the proposed method and the conventional protocol. The myocardium and papillary muscle are well visualized with good contrast in all slices/phases for both protocol, although the small vessels in the liver and lung are slightly better visualized in the conventional CINE. The averaged difference of the calculated blood-pool areas of all slice/phase was 4.7% between the two protocols.Discussion
Our study shows the feasibility of the proposed single breath-hold, ECG-free cardiac CINE, which significantly reduces the complexity of conventional cardiac CINE protocol. The PI-DL algorithm allows high-quality and low-latency image reconstruction of highly under-sampled k-space data and demonstrates the promise of DL in optimizing MR image reconstruction for clinical applications. Future studies will be focused on optimizing the scan protocol and image reconstruction algorithms, as well as systemic validation of the proposed protocol using more clinical datasets.Acknowledgements
No acknowledgement found.References
1. Carr J., Simonetti O., Bundy J., Li D., Pereles S., Finn J. P., Cine MR Angiography of the Heart with Segmented True Fast Imaging with Steady-State Precession. Radiology, 2001;219(3):828–34.
2. Schlemper, J., Caballero, J., Hajnal, J. V., Price, A., & Rueckert, D. A Deep Cascade of Convolutional Neural Networks for MR Image Reconstruction. Information Processing in Medical Imaging (IPMI), 2017.
3. Kerstin Hammernik, Florian Knoll, Daniel Sodickson, Thomas Pock. L2 or not L2: Impact of Loss Function Design for Deep Learning MRI Reconstruction. ISMRM 2017.
4. Uecker M, Lai P, Murphy MJ, Virtue P, Elad M, Pauly JM, Vasanawala SS, Lustig M. ESPIRiT-an eigenvalue approach to autocalibrating parallel MRI: where SENSE meets GRAPPA. Magn Reson Med 2014;71:990–1001.
Figures