1041
Reducing scan time for full MRI examination of the ankle by 45% while maintaining diagnostic value using combined compressed sensing and parallel imaging.1Radiology & Nuclear medicine, Academic Medical Center, Amsterdam, Netherlands, 2Radiologie, Academic Medical Center, Amsterdam, Netherlands, 3Healthcare, Philips, Best, Netherlands
Synopsis
Dixon imaging is a well-known imaging technique that provides robust water-fat separation but requires relatively long acquisition times. We scanned twelve healthy volunteers with a standard ankle examination containing multiple Dixon sequences and an accelerated examination using CS-SENSE, a combination of Parallel Imaging and Compressed Sensing. A five-point Likert scale was used to compare reference images to CS-SENSE images. Although using CS-SENSE caused a slight SNR reduction, the diagnostic value was not impaired. Applying CS-SENSE on an ankle examination protocol resulted in a feasible reduction of the total acquisition time by 45% from 13’38” to 7’49”, without losing diagnostic value.
Introduction
While MRI enables a variety of diagnostic
information, the major limitations remains the relatively long acquisition time
needed compared to other imaging modalities such as CT. For instance, chemical shift-based water-fat
separation, also known as Dixon [1, 2], requires the acquisition of two or
more images at different echo times, which protracts the total scanning time [3]. Dixon is a commonly used MRI technique
in multiple anatomical areas such as musculoskeletal (MSK) and abdominal
imaging. Compared to other methods such as spectral fat saturation, inversion
recovery, and water excitation, Dixon improved the quality of the images and
made quantification possible [1, 4].
To acquire Dixon images in a clinically acceptable scan time, acceleration
techniques, such as parallel imaging and compressed sensing, were introduced. Parallel
Imaging (PI) accelerates data acquisition by undersampling k-space and uses the
sensitivity of phased array coils to reconstruct the missing data [5] [6]. Compressed sensing (CS) uses
incoherent undersampling in k-space. A nonlinear method enforces both sparsity
of the image representation and consistency of the reconstruction [3].
We aimed to determine whether a combination of PI and CS (CS-SENSE) could be
used to accelerate Dixon imaging of the ankle as a model to accelerate MSK
imaging while maintaining similar diagnostic value.
Methods
CS-SENSE enables measuring in a hybrid subsampling pattern of k-space. In the center of k-space regular undersampled patterns are measured. In the outer region of k-space the sampling pattern is measured using pseudo-random sampling and the density drops off at a configurable rate.
Scan protocols of a standard MR examination of the ankle, containing T2 weighted and proton density Dixon sequences, were used as a reference for the feasibility of CS-CSENSE in MSK imaging. Twelve healthy volunteers were scanned on a clinical 3.0T MRI scanner (Ingenia), equipped with a CS-SENSE software prototype extension (Philips Healthcare, Best, the Netherlands). The relevant imaging parameters are listed in table 1.
To determine the diagnostic value of CS-SENSE images compared to standard images, all images were evaluated by two MSK radiology residents (with three and five years of experience, respectively). The images were randomized and blinded to the radiologists. Both scans were presented on two radiology monitors using the RadiAnt DICOM viewer (Medixant, Poznan, Poland). To standardize the assessment, we used a five point Likert scale consisting of 25 scoring questions. (figure 1) The questionnaire included two ligaments of the syndesmosis complex, three ligaments of the lateral complex and six of the deltoid complex. Three tendons of the posteromedial complex compartment were included, three of the anterior compartment and two of the peroneal compartment. For the assessment of the cartilage structures we chose the tibio-talar joint, subtalar joint, calcaneo-cuboid joint and metatarsal joint. For bone structures the trabecula of the talus and calcaneus bone were assessed. Every answer on the Likert scale contributed one point in favor of the preferred type of scan.
Results
The
standard ankle Dixon images had a total acquisition time of 13’38”. The acquisition
times in sagittal, coronal and transverse plane were 3’35”, 4’33” and 5’30”,
respectively. With CS-SENSE these acquisition times were reduced to 2’05”, 2’37”
and 3’07”, respectively. The total acquisition time went from 13’38” to 7’37” a
reduction of 45%.
On the Likert scale, ligaments of the syndesmosis on the CS-SENSE images had
equal diagnostic value compared to the standard Dixon images, just as the
tendons of the posteromedial compartment complex. The two tendons of the
peroneal compartment had an equal diagnostic value in 75% and 25% of the cases in favor of the reference
scan due to higher signal-to-noise ratio (SNR).
Discussion
CS-SENSE imaging provides comparable diagnostic value in 45% less scanning time in the ankle. Although using CS-SENSE caused a slight SNR reduction, this did not impair the diagnostic value. In our institution, Dixon is used in multiple MSK examinations, and we expect that CS-SENSE will achieve a similar scan time reduction in these other regions. CS-SENSE potentially leads to more comfort for our patients and shorter waiting lists and it may benefit health care economics.
Future perspectives
Optimize all Dixon scan protocols, and use CS-SENSE for all anatomies, including advanced and quantitative imaging sequences, such as T2mapping, T1rho, diffusion weighted imaging and diffusion tensor imaging. CS-SENSE may enable quantitative imaging techniques that are currently not commonly used due to impracticable acquisition times.
Conclusion
Initial investigation of applying CS-SENSE in MSK imaging of the ankle shows feasibility of substantial reduction in scan time, while maintaining similar diagnostic value.Acknowledgements
No acknowledgement found.References
References
1. Ma, J., Dixon techniques for water and fat imaging. J Magn Reson Imaging, 2008. 28(3): p. 543-58.
2. Pezeshk, P., A. Alian, and A. Chhabra, Role of chemical shift and Dixon based techniques in musculoskeletal MR imaging. Eur J Radiol, 2017. 94: p. 93-100.
3. Doneva, M., et al., Compressed sensing for chemical shift-based water-fat separation. Magn Reson Med, 2010. 64(6): p. 1749-59.
4. Pezeshk, P., A. Alian, and A. Chhabra, Role of chemical shift and Dixon based techniques in musculoskeletal MR imaging. European Journal of Radiology, 2017. 94(Supplement C): p. 93-100.
5. Pruessmann, K.P., et al., SENSE: sensitivity encoding for fast MRI. Magn Reson Med, 1999. 42(5): p. 952-62.
6. Sodickson, D.K. and W.J. Manning, Simultaneous acquisition of spatial harmonics (SMASH): fast imaging with radiofrequency coil arrays. Magn Reson Med, 1997. 38(4): p. 591-603.
Figures
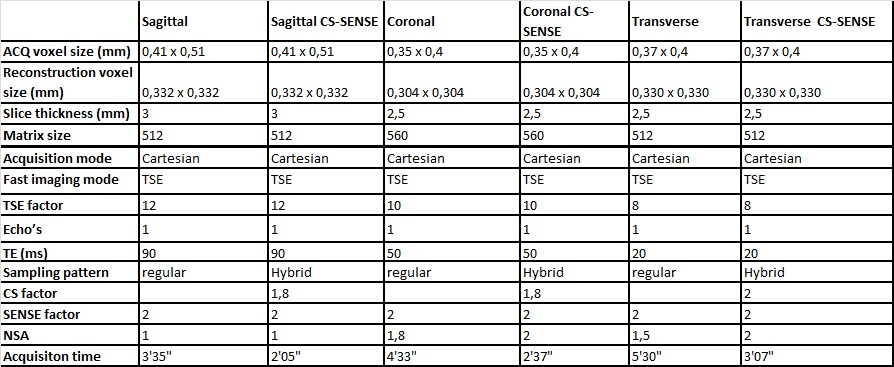
Table 1. Parameters of the sagittal, coronal and transverse plane images with and without CS-SENSE.
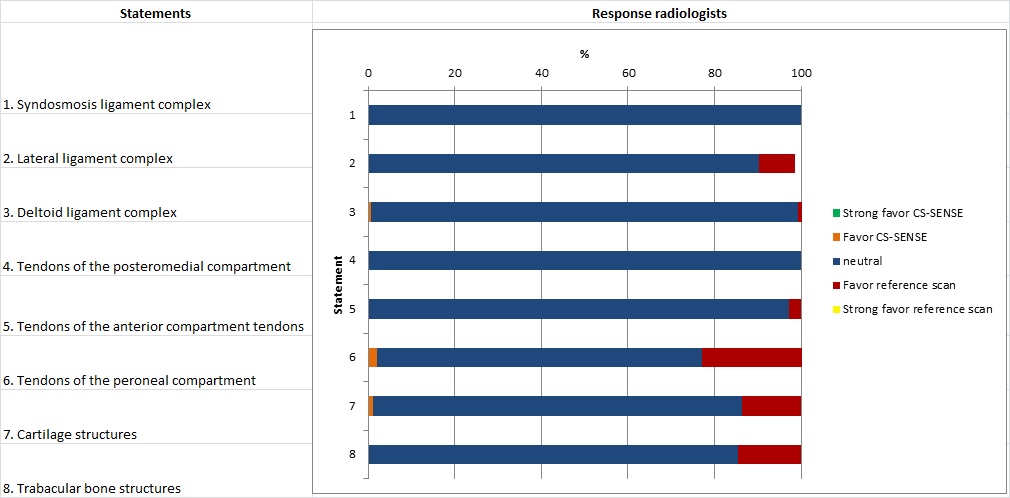
Figure 1. Diagnostic value of the CS-SENSE Dixon scans versus the standard Dixon scans categorized by ligaments, tendons, cartilage and bone structures of the ankle.

Figure 2
On the left the normal Dixon scans are shown and on the right the CS-SENSE
Dixon scans of the ankle. The sagittal
plane (top) is of a fat-only Dixon image, the coronal plane (bottom) is of a
water-only Dixon image.