0967
Hyperpolarized 129Xe Gas Exchange MRI: The Transition from 1.5 to 3 TeslaZiyi Wang1, Mu He2, Elianna Bier3, Brian Soher4, Joseph Mammarappallil4, Sudarshan Rajagopal5, Yuh-Chin Huang6, and Bastiaan Driehuys1,3,4
1Biomedical Engineering, Duke University, Durham, NC, United States, 2Electrical and Computer Engineering, Duke University, Durham, NC, United States, 3Medical Physics Graduate Program, Duke University, Durham, NC, United States, 4Radiology, Duke University Medical Center, Durham, NC, United States, 5Division of Cardiology, Duke University Medical Center, Durham, NC, United States, 6Division of Pulmonary, Allergy and Critical Care, Duke University Medical Center, Durham, NC, United States
Synopsis
Hyperpolarized 129Xe is uniquely suited to imaging pulmonary functions by virtue of its solubility and abundant chemical shifts. Previous efforts established single-breath 3D imaging of 129Xe ventilation, barrier uptake and RBC transfer at 1.5 Tesla. As MR vendors are increasingly transitioning their multinuclear platforms to 3 Tesla, it becomes important to enable 129Xe gas exchange MRI at higher field strengths. Here we demonstrate that by careful measurement of spectral properties and optimization of RF and readout, short T2* can be overcome, and 129Xe gas exchange MRI with quantitative workflow is feasible and robust at 3 Tesla.
INTRODUCTION
Recently, hyperpolarized 129Xe, with its solubility and chemical shifts, has begun to be exploited for pulmonary gas exchange imaging. The first efforts used a multi-echo hierarchical IDEAL approach, 1 and subsequent work used interleaved 3D radial encoding of 129Xe in airspace and dissolved compartments combined with a single-echo 1-point Dixon approach 2 to decompose the barrier and red blood cell (RBC) compartments. To date, these techniques have only been implemented at 1.5 Tesla, due to the short T2* (~2ms) of 129Xe dissolved in alveolar septa. However, with MR vendors increasingly transitioning their multi-nuclear platforms to 3 Tesla, it is essential to establish that 129Xe gas exchange MRI is also feasible at higher fields. The objective of this work was to develop a 3-Tesla implementation for Dixon-based 129Xe gas exchange MRI and to determine optimal acquisition parameters.METHODS
The study enrolled 8 healthy subjects to optimize parameters, and obtained representative images in 4 patients with alpha-1 antitrypsin deficiency (3 MZ and 1 ZZ) and a COPD patient. All imaging was conducted on a 3T Siemens MAGNETOM Trio (VB19). First, in vitro spectroscopy was used to identify the minimum RF sinc pulse duration that could selectively excite dissolved-phase 129Xe without gas-phase contamination. The resulting 0.69 ms 1-lobe pulse was then used to acquire a calibration spectrum that was fit in the time domain to determine the frequency and phase separation between the barrier and RBC resonances, to calculate the TE of barrier and RBC being 90° out of phase. The TE90 and sinc pulse were used to acquire 1000 interleaved 3D-radial gas and dissolved views, with flip-angles = 0.5/20°, TR = 7.5ms and FOV = 36cm3 (Figure 1). Each view had 64 points, acquired at 399Hz/pixel (2.5ms read-out). Each readout gradient was carefully timed to ensure the first point was acquired at k=0 and each was followed by an x-gradient crusher to dephase the gas-phase residual magnetization. After image encoding, a singled dissolved-129Xe spectrum was acquired to derive the global, steady-state RBC:Barrier ratio corresponding to this flip angle and effective 15ms dissolved-phase TR. All imaging was done with patients inhaling an effective 129Xe dose of ~110 ml. 3 The reconstructed dissolved-phase image was phase-shifted to align RBC and barrier to real and imaginary channels such that their intensity ratio matched the RBC:Barrier from the spectrum. The images were processed as previously described. 4RESULTS
Figure 1(c)(d) shows the consumption of gas and dissolved-phase magnetization over the acquisition. Figure 2 shows the effect of tuning sinc pulse duration on off-resonance gas-phase excitation. The optimum of 0.69ms generating a tolerable 3% contamination in vivo. Figure 3 shows the chemical shift of the dissolved-phase resonance for 2 representative healthy subjects as well as the line-shape parameters of the healthy cohorts at 1.5 vs. 3 Tesla. At 3T (34.092MHz gas-phase), the RBC and barrier resonance are at 217.5 ± 0.5 ppm and 197.9 ± 0.2 ppm, with linewidths 8.5 ± 0.4 ppm and 7.7 ± 0.3 ppm respectively. The RBC linewidth suggests a lower bound of T2* ~1.2ms. Figure 4 shows representative reconstructed images of a patient with longitudinal scans at both 1.5T and 3T, 21 months apart. Figure 5 shows the processed color maps of the same patient. Both images show mild ventilation defects and enhanced barrier uptake, but most notably, a prominent RBC transfer defect is visualized on both images.DISCUSSION
These preliminary results indicate that 1-point Dixon-based imaging of 129Xe gas exchange is feasible at 3-Tesla. Selective excitation of dissolved-phase 129Xe benefits from the larger chemical shift and was enabled with a simple 0.69ms 1-lobe sinc pulse. This enabled k = 0 to be acquired at roughly TE = 0.45ms where RBC and barrier are 90° out of phase. Analysis of the dissolved line-shapes suggests T2* ~1.2ms, which was managed with a 2.5ms read-out. Despite the short T2* of the dissolved resonances, the gas-phase resonance T2* was estimated to be ~8ms, making it important to crush its transverse magnetization. This work incorporated several improvements to the initial published method. 4 First, the spectrum for determining the RBC:Barrier ratio was now acquired as part of the imaging sequence, ensuring it reflected the steady-state conditions as the image. Secondly, the radial view randomization ensures that the sequence is robust against potential early exhalation by patients with compromised pulmonary function. Initial estimates suggest that image SNR is comparable to 1.5 Tesla, while several aspects remain to be further optimized. Based on these preliminary results, it appears that 129Xe gas exchange imaging can be deployed to high field clinical scanners.Acknowledgements
R01HL126771, R01HL105643, P41 EB015897, Gilead Sciences, Duke MITPReferences
- Qing, K., et al., Regional Mapping of Gas Uptake by Blood and Tissue in the Human Lung Using Hyperpolarized Xenon-129 MRI. Journal of Magnetic Resonance Imaging, 2014. 39(2): p. 346-359.
- Kaushik, S.S., et al., Single-breath clinical imaging of hyperpolarized (129)Xe in the airspaces, barrier, and red blood cells using an interleaved 3D radial 1-point Dixon acquisition. Magn Reson Med, 2016. 75(4): p. 1434-43.
- He, M., et al., Dose and pulse sequence considerations for hyperpolarized (129)Xe ventilation MRI. Magn Reson Imaging, 2015. 33(7): p. 877-85.
- Wang, Z., et al., Quantitative analysis of hyperpolarized 129 Xe gas transfer MRI. Med Phys, 2017. 44(6): p. 2415-2428.
Figures
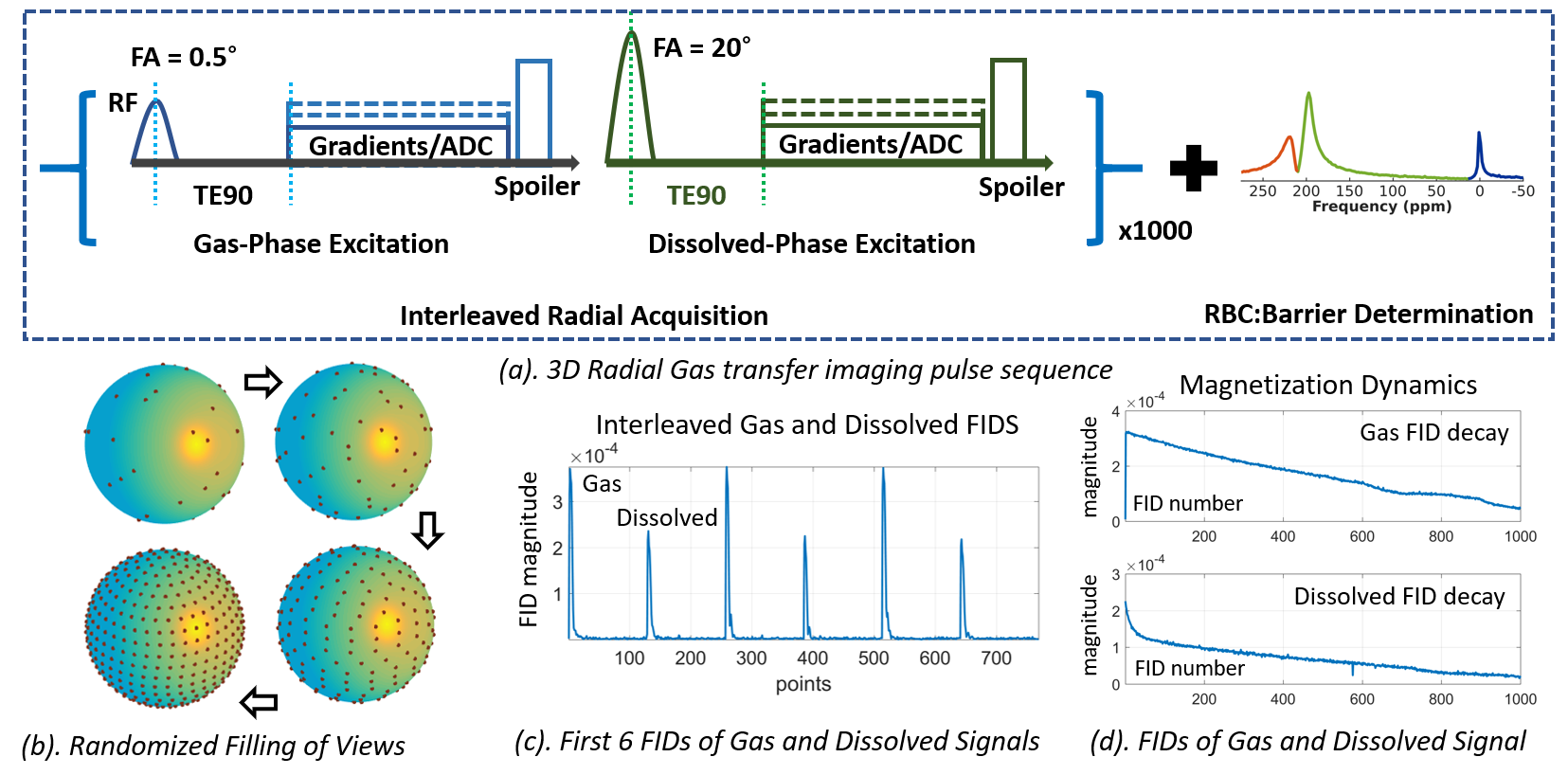
Figure 1 (a).
The 3D radial sequence consists of 1000 interleaved radial acquisitions of gas-
and dissolved-phase signals, with identical imaging parameters except flip
angle (0.5° for gas and 20° for dissolved). A single dissolved-phase
spectrum is appended to the end of imaging to capture the global RBC:Barrier
ratio. (b). The randomized-spiral trajectory converges to an even sampling
pattern once all 1000 views are acquired. (c). Interleaved dissolved and gas FIDs
show roughly equal amplitudes despite being acquired with 40x different flip
angles. (d). Signal decay of the 1000 gas and dissolved FIDs, showing that
magnetization is nearly fully consumed.
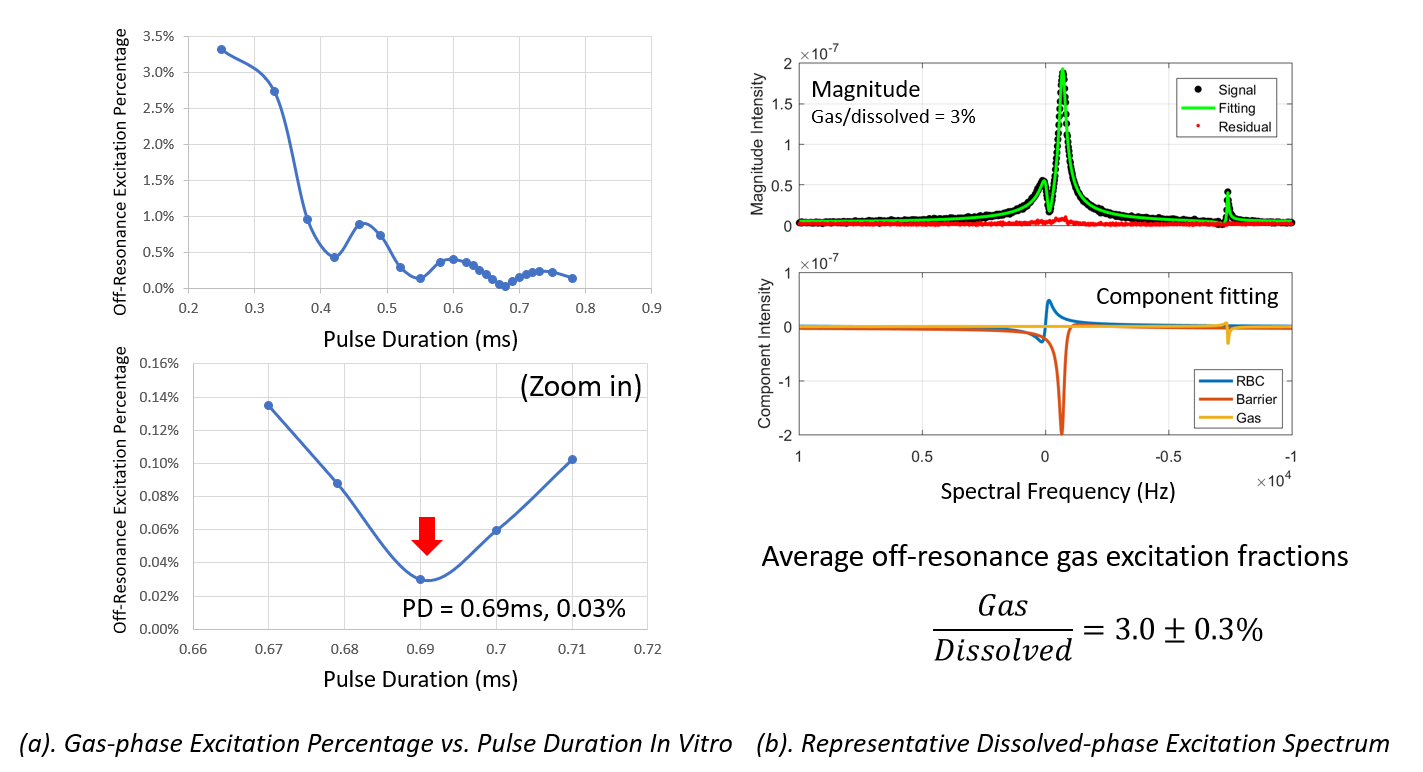
Figure 2 (a).
Off-resonance gas excitation vs. pulse duration tested with 1H signal
and verified with 129Xe using the shared extremity coil/MNS RF power
amplifier. 0.69ms was found for minimal off-resonance excitation in
vitro. (b). Representative dissolved-phase spectrum of one healthy subject and
curve-fitting of the 3 components (RBC, barrier, and gas). Off-resonance excitation
is 3% of dissolved signal. The average gas excitation for all subjects was a
tolerable 3.0 ± 0.3% of the magnitude of dissolved-phase signals.
The higher off-resonance excitation in vivo is likely caused by the broader
gas-phase linewidth in lungs vs phantoms (40Hz vs 5 Hz).
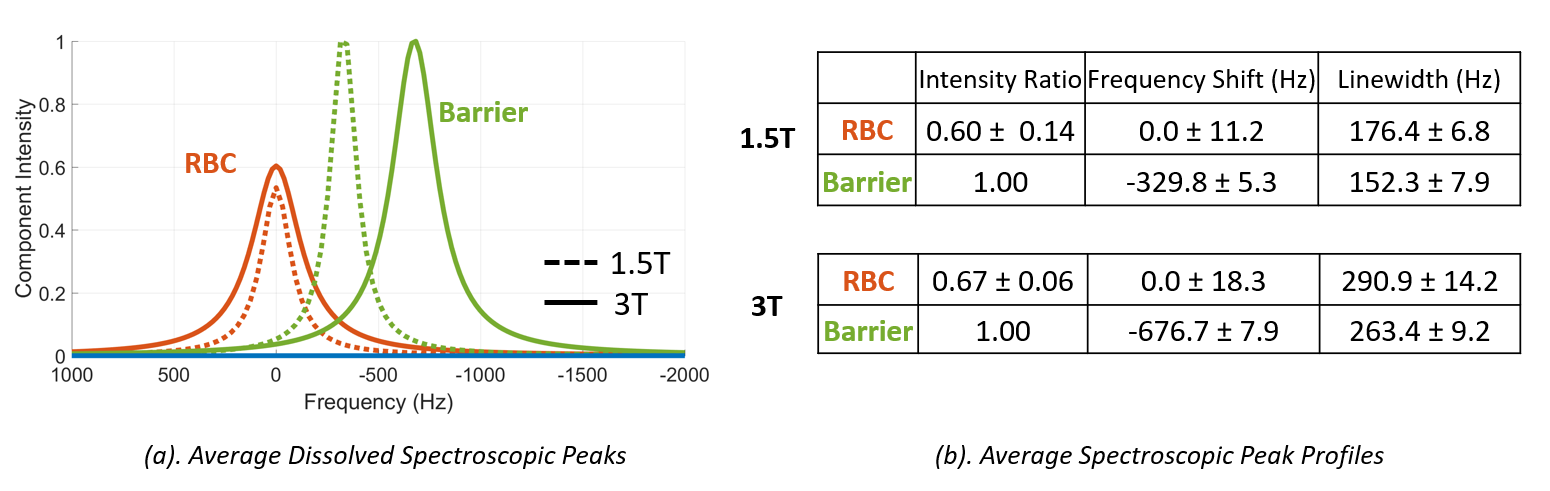
Figure 3 (a).
The normalized spectroscopic fitting of RBC and barrier of 2 representative
healthy subjects at 1.5T and 3T. The absolute chemical shift is doubled at 3T,
as would be expected. (b). The average spectroscopic line-shape parameters of the
healthy cohort at 1.5T and 3T. The linewidths of both components at 3T are
slightly smaller than what might be predicted by doubling those measured at 1.5T.
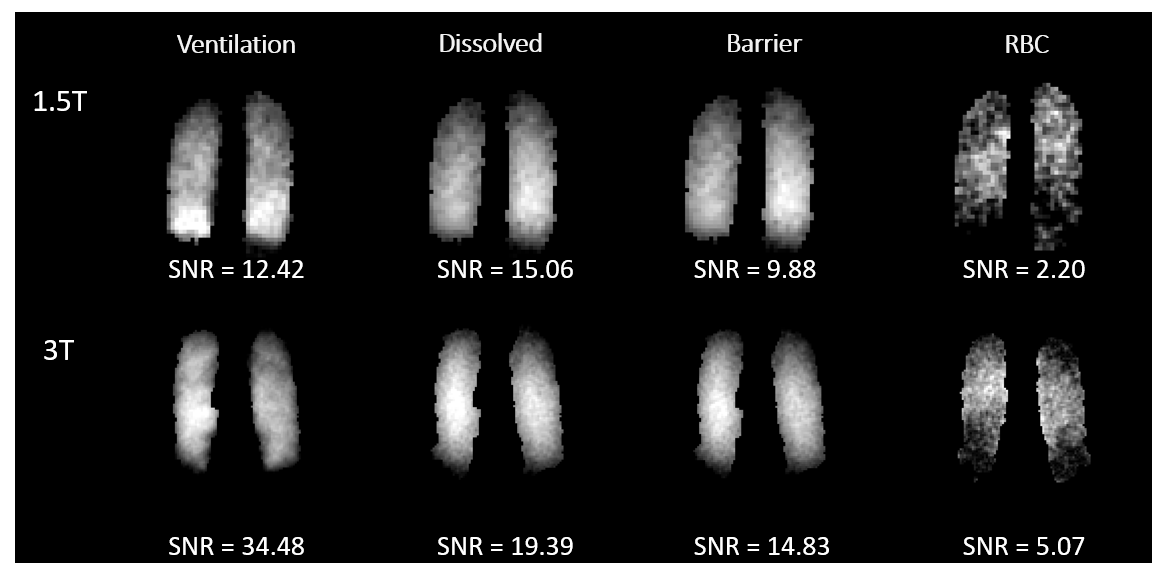
Figure 4 Representative
raw ventilation, dissolved, and decomposed barrier and RBC images from an alpha-1
antitrypsin heterozygote patient scanned at both 1.5 Tesla and 3 Tesla (21 months apart). The images at 3 Tesla achieved higher SNR.
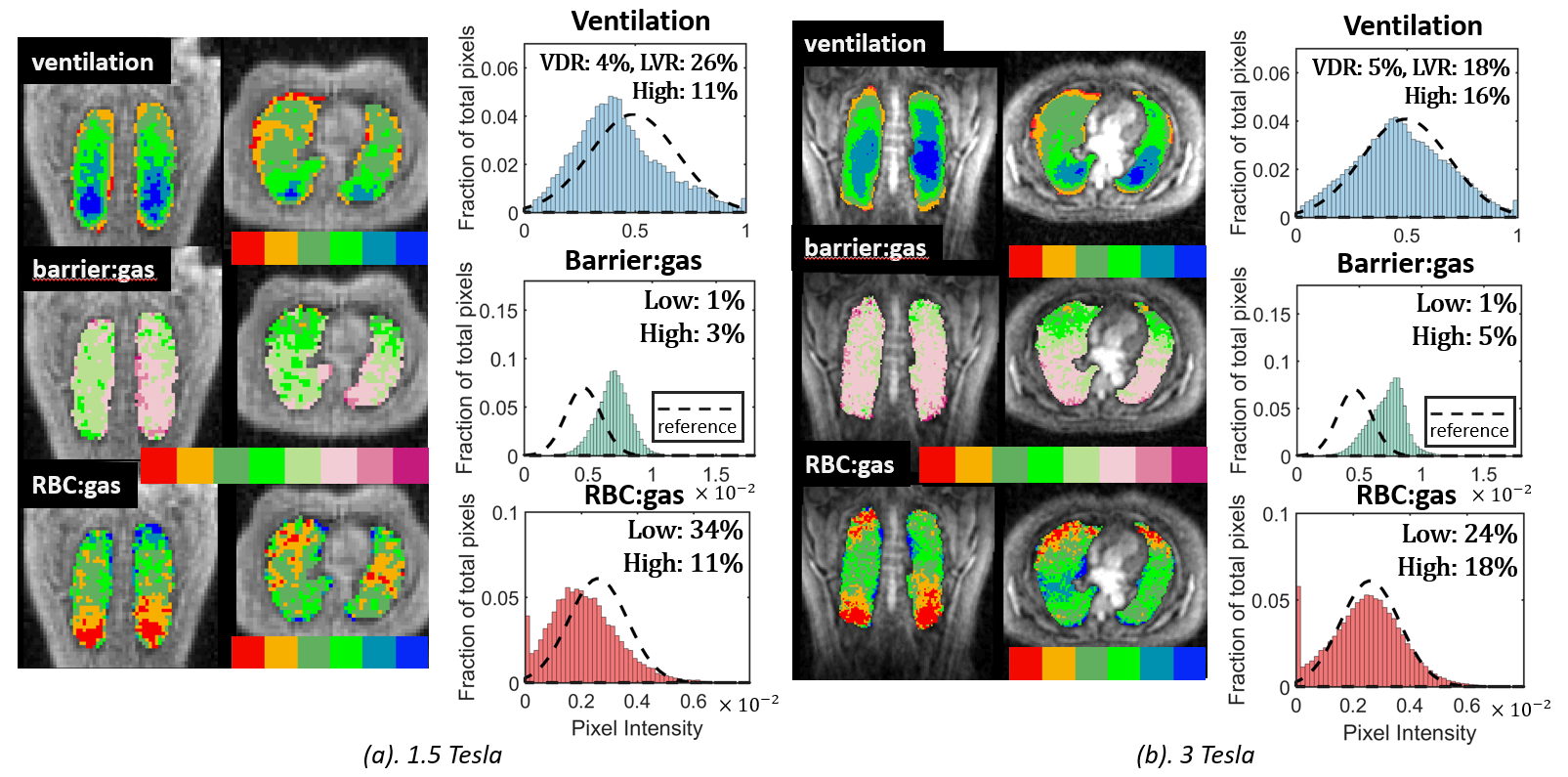
Figure 5 Representative
ratio maps of the alpha-1 antitrypsin heterozygote patient processed according
to the quantitative workflow 4 at both field strengths. At 3 Tesla follow-up,
the patient shows slightly improved ventilation and moderately increased Barrier:Gas
ratio. A distinct RBC transfer defect in the basal lung of the coronal view is
readily visualized on both the 1.5 Tesla and 3 Tesla scans.