0921
Accuracy of ECG-triggered Non-contrast Enhanced MRA (TRANCE) versus CT Angiography for diagnosis of peripheral artery disease: Comparison with DSA1MRI, The 1st affiliated hospital of Henan University of TCM, Zhengzhou, China, 2PHILIPS Healthcare, Beijing, China
Synopsis
There is an increasing clinical need for implementing a Non-contrast enhanced MRI technique for patients with PAD or contraindications for the use of contrast medium, especially patients with renal insufficiency. We optimized TRANCE with best performance at 3.0T and compared image quality and diagnostic accuracy versus CTA and DSA for evaluation of low extremity PAD.
INTRODUCTION
Although DSA is the reference standard for detecting peripheral artery disease (PAD) of lower extremities, more sophisticated noninvasive imaging may be necessary for further anatomic delineation and treatment planning, especially before revascularization. Both CT angiography (CTA) and contrast-enhanced MRA (CE-MRA) are rated as “usually appropriate” diagnostic approaches for claudication with suspected vascular etiology. Patients with PAD frequently experience several comorbidities, which often increases the risk regarding the administration of either iodinated or gadolinium-based contrast agents in view of iodinated contrast-induced nephropathy and nephrogenic systemic fibrosis (NSF). Thus, MR imaging without gadolinium-based contrast agents is preferred and non-contrast enhanced MR angiography (NCE-MRA) gained more clinical interest. TRANCE technique is a cardiac triggered 3D TSE technique that subtracts images from different phases in the cardiac cycle to obtain high resolution arterial images with bright vessels and dark background. TRANCE has been optimized for best performance at 1.5T, but seldom used at 3.0T. The purpose of this study was to prospectively evaluate the image quality and diagnostic value of TRANCE in patients with PAD in comparison to CTA against DSA as being the pre-interventional standard of reference before treatment.
METHODS
A total of 45 patients with PAD underwent lower extremity CTA and NCE-MRA with TRANCE technique. DSA was performed within 30 days. MRA examinations were performed on a 3.0 T (Ingenia, PHILIPS, Netherlands) with surface coil. Before staring NCE-MRA, we performed a phase contrast sequence(Q-flow) acquisition of every stack. The parameters for TRANC: TR/TE 1.8ms/3.3ms,NSA 1,FOV 380mm×380mm,thickness 1.1mm,Flip angle 90°. The CTA was performed on a third generation dual source CT system (Somatom Definition Force, Siemens, Germany) in dual-energy mode. Iodinated contrast was administered intravenously with a multiphasic injection. The parameters for CTA: FOV 350mm, pitch 0.7, collimation 2×64×0.6mm. Two independent observers performed image assessments of TRANCE and CTA. Image evaluation was performed on a per-segment basis according to an 18-segment model. The overall image quality was rated independently by 2 observers according to a 3-point grading system and arterial stenoses were graded using a 5-point grading scale. Differences in significant stenosis of TRANCE and CTA were analyzed with a chi-square test and correlation between 2 observers was evaluated using ICC.The diagnostic sensitivity and specificity were calculated on a per-segment basis.The inter-observer agreement in image quality scores were analyzed by Cohen’s Kappa test.RESULTS
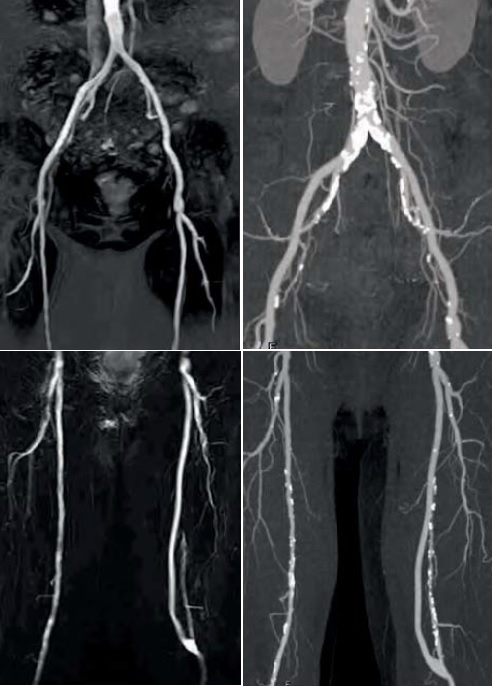
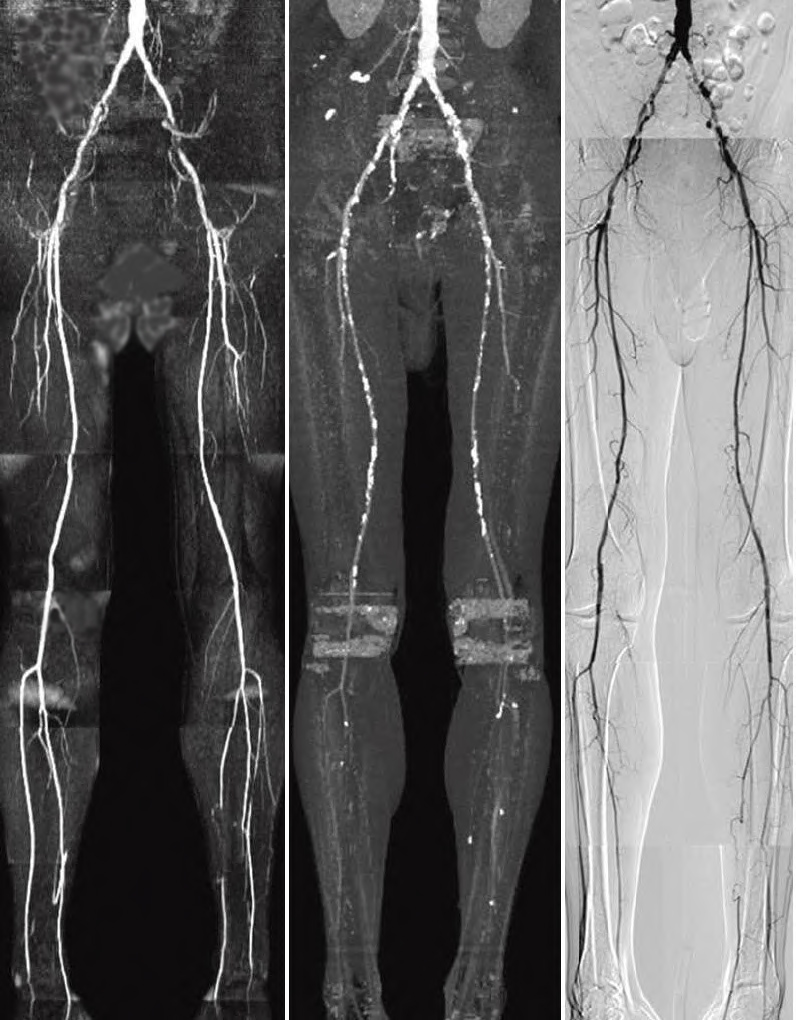
A total of 540 segments were imaged by TRANCE and CTA. Overall image quality was rated similarly with TRANCE (2.65) and CTA (2.58). Interobserver agreement in TRANCE and CTA ratings was good to excellent for the overall image quality (ICC 0.78 and 0.81). Of the 540 segments, >50% stenosis was detected by TRANCE, CTA and DSA in 140(26%), 162(30%),172(32%) segments, respectively. No difference between the stenosis detection rates of TRANCE and CTA was observed. The ICC analysis showed good agreement between TRANCE and CTA (0.80). The sensitivity and specificity for the detection of >50% stenosis by TRANCE and CTA are 86.5% and 87.4%, 95.6% and 94.3%, respectively. Interobserver agreement regarding the detection >50% stenosis was excellent for TRANCE(k=0.81) and CTA(k=0.83). DISCUSSION TRANCE is cardiac triggered 3D TSE technique that subtracts images from different phases in the cardiac cycle to obtain high resolution arterial images with bright vessels and dark background. TRANCE background suppression is mostly excellent and it could be very easily seen collateral blood circulation. TRANCE is compatible with large FOV (380 to 450 mm) and high matrix sizes with scan time. High-resolution TRANCR provides 1.5mm section thickness and a more detailed visualization of the vascular anatomy. TRANCE showed high sensitivity and specificity and detection rate of> 50% stenosis based on TRANCE similar to that of CTA. Image quality was rated subjectively by 2 observers and TRANCE was found to provide similar vascular signal to that of CTA. Stenosis grading based on TRANCE showed good agreement with DSA. Nearly 90% of the segments were graded properly by TRANCE, similar to CTA, indicating that TRANCE can potentially be used for stenosis severity assessment. Such an accurate non-contrast MRA approach has particular benefits in the pre-procedural diagnostic workup of PAD patients with an elevated medical risk profile.CONCLUSIONS
The study indicates that non-contrast MRA yields a high diagnostic accuracy and image quality with good to excellent agreement for depiction of stenosis and occlusion for lower extremities arteries in patients with PAD. TRANCE is a feasible alternative to CTA and DSA for patients with renal insufficiency or contraindication to contrast agents.Acknowledgements
Contract grant sponsor: Traditional Chinese Medicine Research Project of Henan Province of China. Contract grant number: 2015ZY02014References
Wheaton AJ, Miyazaki M. Non-contrast enhanced MR angiography: physical principles. J Magn Reson Imaging 2012;36:286–304.
Bonel H M, Saar B, Hoppe H, et al. MR Angiography of Infrapopliteal Arteries in Patients with Peripheral Arterial Occlusive Disease by Using Gadofosveset at 3.0 T: Diagnostic Accuracy Compared with Selective DSA 1[J]. Radiology, 2009, 253(3): 879-890.
Fan Z, Sheehan J, Bi X, et al. 3D noncontrast MR angiography of the distal lower extremities using flow‐sensitive dephasing (FSD)‐prepared balanced SSFP[J]. Magnetic resonance in medicine, 2009, 62(6): 1523-1532.
Offerman E J, Hodnett P A, Edelman R R, et al. Nonenhanced methods for lower‐extremity MRA: A phantom study examining the effects of stenosis and pathologic flow waveforms at 1.5 T[J]. Journal of Magnetic Resonance Imaging, 2011, 33(2): 401-408.
Liu X, Fan Z, Zhang N, et al. Unenhanced MR angiography of the foot: initial experience of using flow-sensitive dephasing–prepared steady-state free precession in patients with diabetes[J]. Radiology, 2014, 272(3): 885-894.
Wheaton A J, Miyazaki M. Non‐contrast enhanced MR angiography: Physical principles[J]. Journal of Magnetic Resonance Imaging, 2012, 36(2): 286-304.
Fan Z, Hodnett PA, Davarpanah AH, et al. Non-contrast magnetic resonance angiography of the hand: improved arterial conspicuityby multidirectional flow-sensitive dephasing magnetization preparation in 3D balanced steady-state free precession imaging. Invest Radiol 2011;46:515–523.
Figures