0918
Whole-Heart Cartesian Coronary MRA with Sub-Millimeter Isotropic Resolution in Four-Minute Acquisition1Biomedical Engineering Department, King's College London, London, United Kingdom, 2Siemens Healthcare Limited, Frimley, United Kingdom
Synopsis
Whole-heart coronary magnetic resonance angiography (CMRA) with isotropic resolution allows reformatting in any desired imaging plane without loss of resolution. However, achieving sub-millimeter isotropic resolution with a conventional 1D diaphragmatic navigator gated CMRA is very challenging due to long and unpredictable scan times. In this study, we sought to achieve sub-millimeter CMRA by combining 2D image-based navigator motion correction with highly accelerated compressed sensing reconstruction in concert with variable density Cartesian spiral-like k-space sampling to significantly accelerate the scan. The proposed technique enables CMRA acquisitions with 0.9mm isotropic spatial resolution in about 4 minutes. Ultimately, this technique might be useful for rapid screening of the coronaries in patients with suspected coronary artery disease.
PURPOSE
Whole-heart high-resolution isotropic coronary magnetic resonance angiography (CMRA) allows image reformatting in any desired imaging plane without loss of resolution, providing detailed information on the integrity of the coronary arteries and surrounding vessels. However, achieving sub-millimeter isotropic resolution with a conventional 1D diaphragmatic navigator (dNAV) gated Cartesian CMRA is very challenging due to prohibitively long and unpredictable scan times. A 2D image-based navigator (iNAV) has been proposed as an alternative to dNAV resulting in 100% scan efficiency and a two-fold reduction in total scan time.1 In this study, we sought to achieve sub-millimeter Cartesian CMRA in a clinically feasible scan time by combining 2D iNAV with a highly accelerated variable density Cartesian spiral like sampling (VD-CASPR2) in concert with a compressed sensing (CS) reconstruction.3METHODS
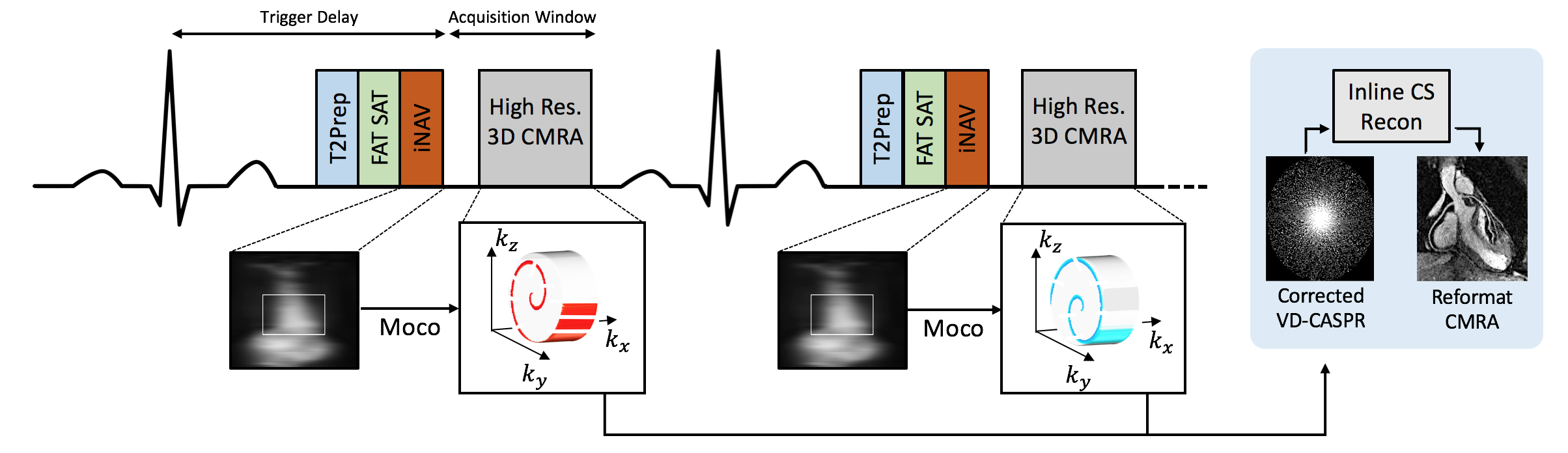
A prototype undersampled variable density CASPR sampling was implemented on a 1.5T scanner (Magnetom Aera, Siemens Healthcare). VD-CASPR samples the ky-kz phase-encoding plane following approximate spiral interleaves on the Cartesian grid with variable density along each spiral arm (Fig. 1). The undersampling scheme was developed such that high acceleration induces “noise-like” incoherent artefacts and avoids strong image disturbance from fold-over artefacts. A 2D iNAV precedes each spiral acquisition to enable beat-to-beat 2D translational respiratory motion estimation without any data rejection. A template-matching algorithm was used to estimate superior-inferior and right-left translational motion, using end-expiration as respiratory reference position.1 Wavelet-based CS reconstruction3 with 2D translation motion correction (k-space linear phase shifting) was implemented and integrated in the Gadgetron framework4 for direct in-line reconstruction.
Imaging:
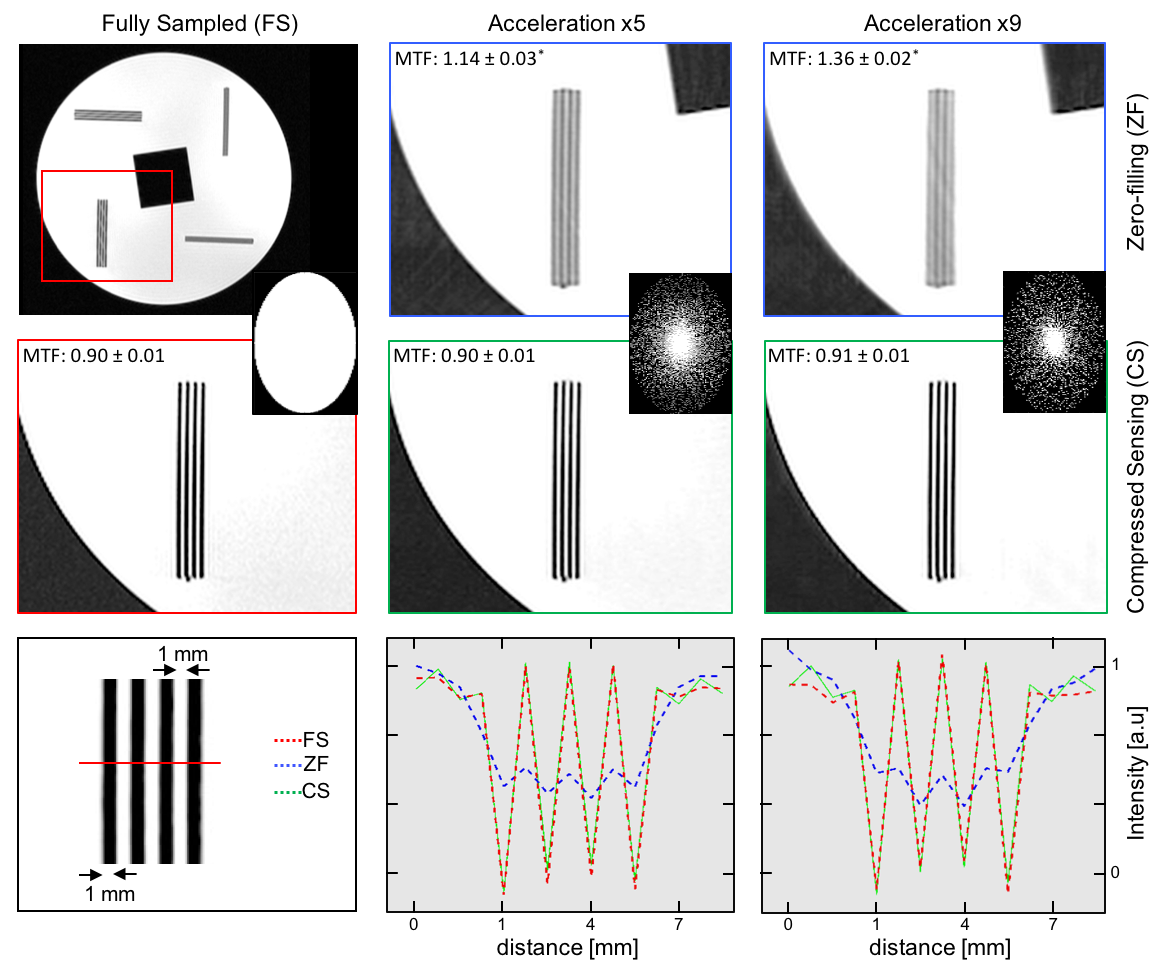
Phantom - A resolution phantom, composed of parallel bar patterns with in-plane resolution of 1mm, was scanned using VD-CASPR. Acquisitions were performed with full k-space sampling and with acceleration factors of 5 and 9. Scan parameters included: 3D bSSFP acquisition, TR/TE=3.7/1.63ms, FA=90°, Bandwidth=890 Hz/pixel, T2-preparation duration=40ms, FOV=306x306x80mm3, and 0.9mm3 isotropic resolution. The acquired data were reconstructed using CS. The modulation transfer function (MTF) was used to help understand how acceleration affects the reconstructed resolution, and was directly obtained by taking the Fourier transform of ten line spread functions (first derivative of the edge response) in the image. The reconstructed resolution was given by the value of the MTF at 10%.
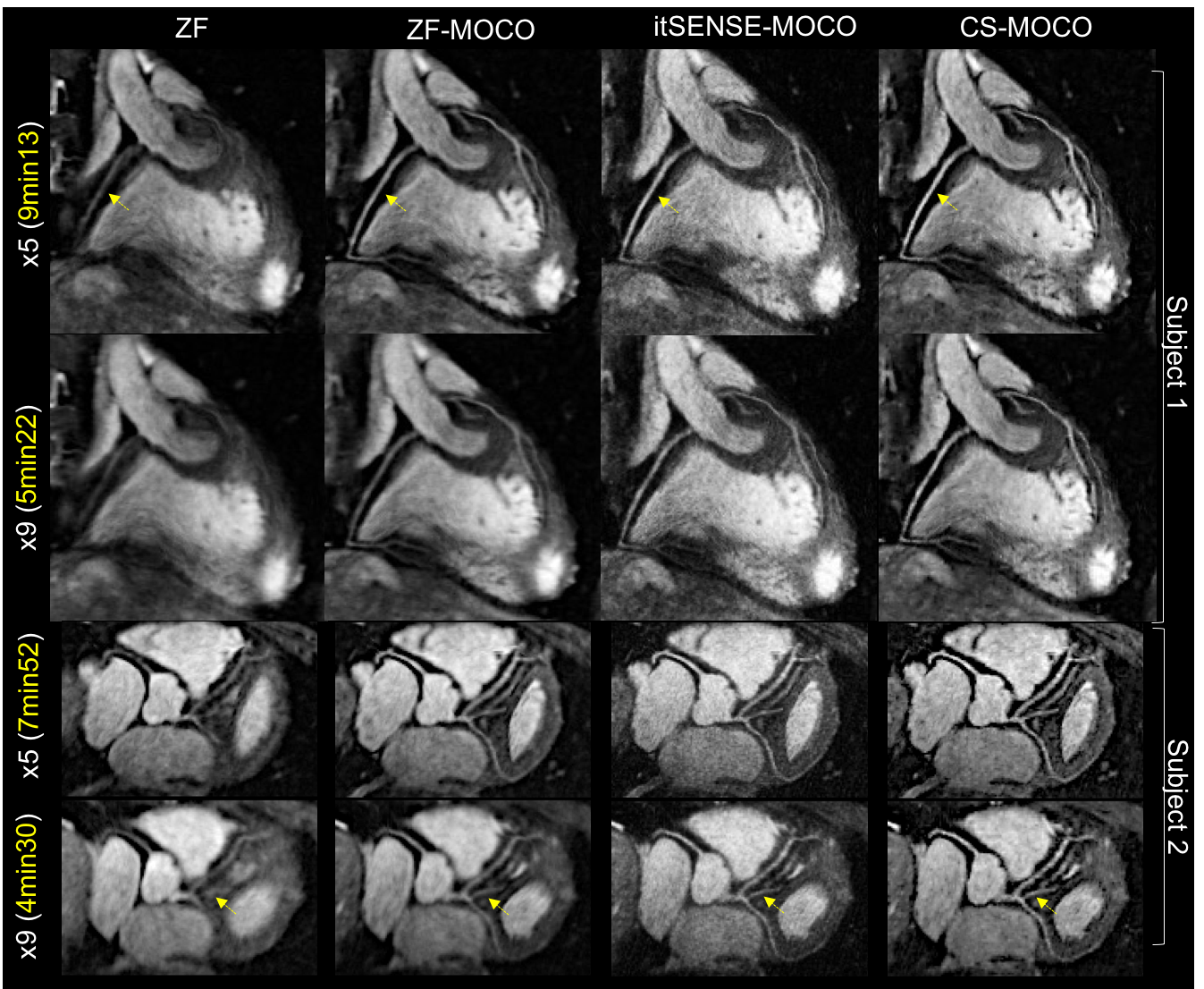
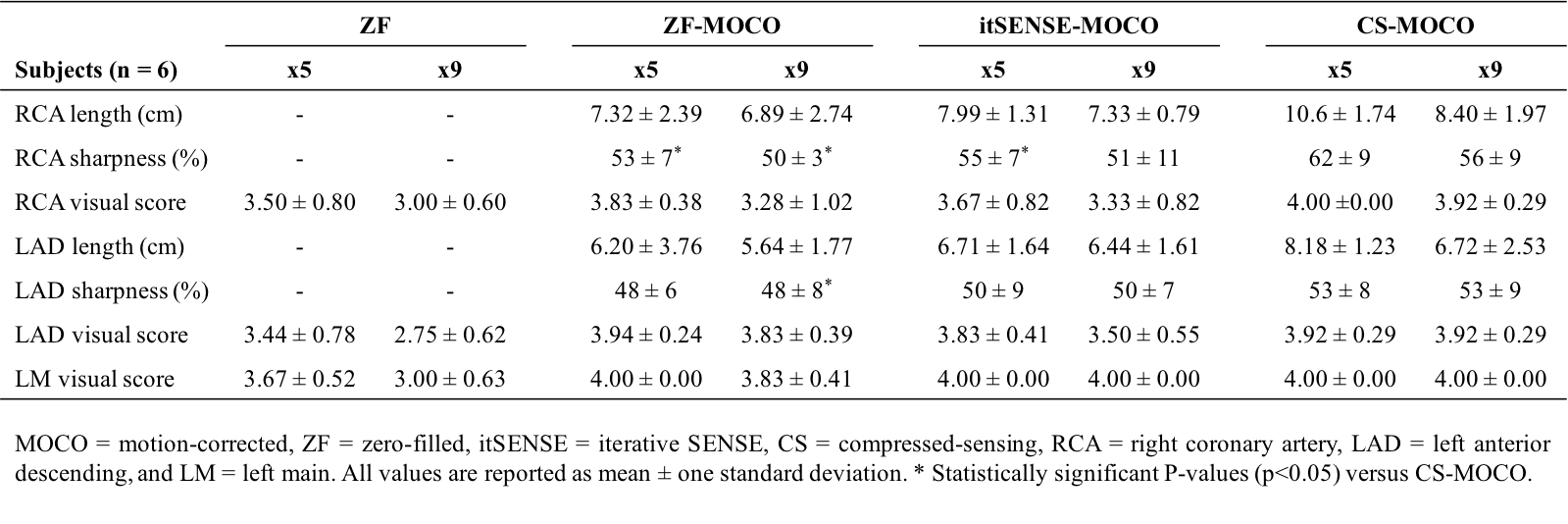
In vivo - Six healthy subjects (4 females, 29±3 years) underwent free-breathing CMRA. Data were acquired without respiratory gating (100% scan efficiency) with an ECG-gated bSSFP sequence, 18-channel body and 32-channel spine coils, mid-diastolic subject-specific acquisition window (range ~90-125ms corresponding to ~30 k-space lines acquired per cardiac cycle), fat-saturation, FOV=320x320x160mm3, same TR/TE/FA/T2-preparation, with 0.9mm3 isotropic resolution and undersampling factors of 5 and 9 (resulting in ~10x and ~18x acceleration in comparison to fully sampled dNAV CMRA with ~50% scan efficiency). The proposed approach was compared to conventional zero-filled (ZF) and iterative SENSE (itSENSE5) reconstructions. Two blinded cardiologists scored the image quality and vessel sharpness and length of the right (RCA) and left (LAD) coronary arteries were measured.6
RESULTS
A fixed number of 30 iterations was used for the CS reconstruction (5 for itSENSE).The average total reconstruction time was ~7min on the scanner computer. Phantom - The reconstructed undersampled images are shown in Figure 2 in comparison with the fully-sampled image. Reconstructions with acceleration factors of 5 and 9 provided excellent visual agreement with the reference fully sampled image. The spatial resolution, as quantified by the MTF, was preserved with the proposed reconstruction. In vivo - The average acquisition time was 7min±17s (x5) and 4min±17s (x9) with 100% respiratory scan efficiency. Sub-millimeter imaging results in clear depiction of the left and right coronary systems and their thin surrounding vessels (Figure 3). The ZF reconstructions with VD-CASPR exhibit incoherent artefacts that behave like random noise and blurring. Blurring is reduced after motion correction and sharpness is further improved with itSENSE. The proposed motion corrected CS reconstruction led to further improvements in terms of vessel sharpness and vessel length for both acceleration factors (Figure 4 and Table 1). Visual and subjective image quality scores demonstrate that the proposed approach is robust even at high acceleration factors.DISCUSSION
We demonstrate the feasibility of combining an efficient VD-CASPR sampling trajectory with 2D iNAV-based motion correction and CS reconstruction to obtain isotropic sub-millimeter CMRA under free-breathing conditions with an acquisition time of ~4 minutes. The proposed technique reduces scan time of sub-millimeter CMRA to predictable and clinically tolerable durations. This technique may be useful for rapid screening of the major coronary vessels in patients with suspected coronary artery anomalies. Future studies will assess its utility for the identification of stenotic coronary artery disease.Acknowledgements
This work was supported by an EPSRC programme and project Grant (EP/P001009/1 and EP/P007619/1) and FONDECYT N° 1161051.References
1. Henningsson M, et al. Whole-heart coronary MR angiography with 2D self-navigated image reconstruction. Magnetic resonance in medicine. 2012;67(2):437-45.
2. Prieto C, et al. Highly efficient respiratory motion compensated free-breathing coronary MRA using golden-step Cartesian acquisition. Journal of magnetic resonance imaging. 2015;41:738-46.
3. Lustig M, et al. Sparse MRI: The application of compressed sensing for rapid MR imaging. Magnetic resonance in medicine. 2007;58(6):1182-95.
4. Hansen MS, Sorensen TS. Gadgetron: an open source framework for medical image reconstruction. Magnetic resonance in medicine. 2012;69:1768-76.
5. Pruesmann KP, et al. Advances in sensitivity encoding with arbitrary k-space trajectories. Magnetic resonance in medicine. 2001;46(4):638-651.
6. Etienne A, et al. “Soap-Bubble” visualization and quantitative analysis of 3D coronary magnetic resonance angiograms. Magnetic resonance in medicine. 2002;48(4):658-66.
Figures