0914
Ferumoxytol-Enhanced 4D MUSIC: Early Multi-Center Experience on Value-Added Magnetic Resonance Imaging in Pediatric Congenital Heart Disease1Department of Radiological Sciences and Medicine, David Geffen School of Medicine at UCLA and VA Greater Los Angeles Healthcare System, Los Angeles, CA, United States, 2Department of Medical Imaging, Ann & Robert H. Lurie Children's Hospital of Chicago, Chicago, IL, United States, 3Division of Cardiology, Children's Hospital of Philadelphia, Philadelphia, PA, United States, 4Department of Radiological Sciences, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States, 5Department of Radiological Sciences and Medicine, David Geffen School of Medicine at UCLA, Los Angeles, CA, United States
Synopsis
The value of MRI in congenital heart disease (CHD) is well-recognized. However, high time overhead and the requirement for expert oversight of image acquisition impede its more widespread use. Ferumoxytol-enhanced 4-dimensional multiphase imaging with contrast (4D-MUSIC) is a cardiac phase-resolved MR technique that generates highly detailed images under controlled ventilation. Our early multi-center experience demonstrates that 4D-MUSIC provides value-added imaging in CHD by shortening the examination time, simplifying the imaging protocol, and providing reliable, gadolinium-free, high spatial resolution, cardiac phase-resolved images. When combined with locally available velocity mapping, 4D-MUSIC enables comprehensive imaging of complex CHD in less than 40 minutes.
INTRODUCTION:
Although the value of magnetic resonance imaging (MRI) in complex congenital heart disease (CHD) is clear, long examination times and the need for expert oversight of image acquisition limit its more widespread use. At the same time, recent findings of gadolinium (Gd) retention in brain and bone have resulted in more cautious use of Gd-enhanced MRI, particularly in small children who will likely undergo repeated imaging over the course of their lifetime. Ferumoxytol-enhanced (FE) 4-dimensional multiphase imaging with contrast (4D-MUSIC) is a cardiac phase-resolved MR technique that enables acquisition of respiratory gated, 3D high spatial resolution images under controlled ventilation1, 2. Ferumoxytol (Feraheme®, AMAG Pharmaceuticals) is a superparamagnetic iron oxide nanoparticle used for treatment of iron deficiency anemia secondary to chronic kidney disease. Because of its long intravascular half-life and high MR relaxivity3, 4, ferumoxytol is uniquely effective in supporting steady state image acquisition. We have shown that FE 4D-MUSIC provides highly diagnostic images5 combining volumetric and functional quantification1, and adds value in the care of patients with CHD at a single institution5. We aim to demonstrate that the reliability and value of 4D-MUSIC in complex CHD are applicable across several academic medical centers.METHODS:
In this IRB-approved study, 4D-MUSIC was implemented in three academic medical centers, and at two field strengths. Due to the heterogeneity of CHD, we categorized CHD into 3 subtypes: Group 1-simple CHD (native /repaired, cared for by the general medical community), Group 2-CHD of moderate severity (seen periodically at regional CHD centers), Group 3-CHD of great complexity (seen regularly at CHD centers)6. Ferumoxytol was diluted and administered by IV infusion to a total dose of 4mg/kg. Vital signs were continuously monitored. Typical image acquisition parameters were: TR/TE 2.9/0.9 ms, FA 25°, 3D isotropic resolution 0.6-0.9mm (true acquired resolution), GRAPPA 2-3X, 75% partial Fourier for phase and partition encoding directions. Ten to 20 cardiac phases were acquired. Local investigators evaluated the image quality and artifacts. We assigned one point for each measure of value (maximum value-added score of 5): shortened the overall exam time, alleviated concerns about Gd retention, precluded the need for renal function testing, simplified the image acquisition workflow, and achievement of similar or better image quality compared to the MRI standard of care at the local institution.RESULTS:
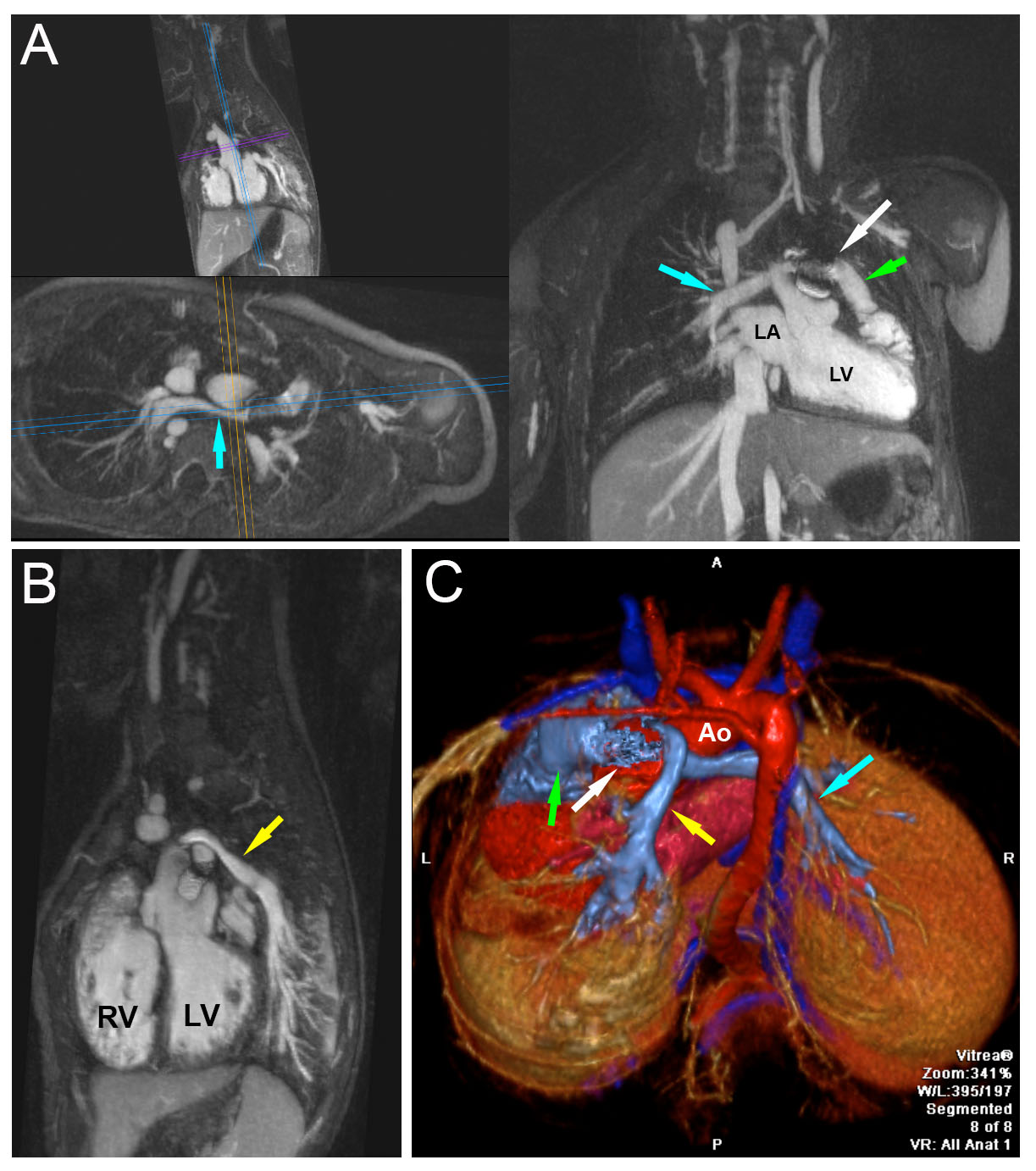
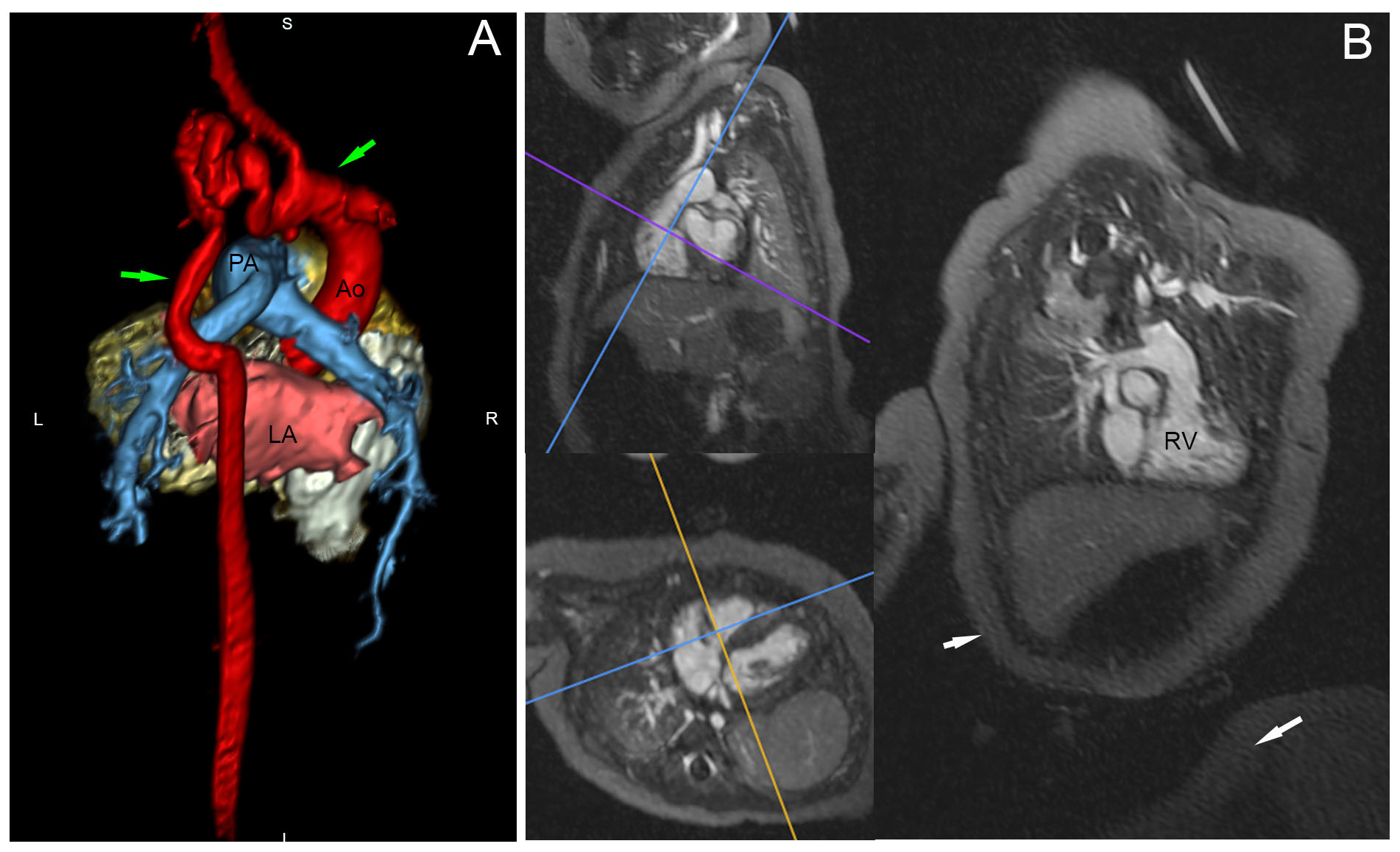
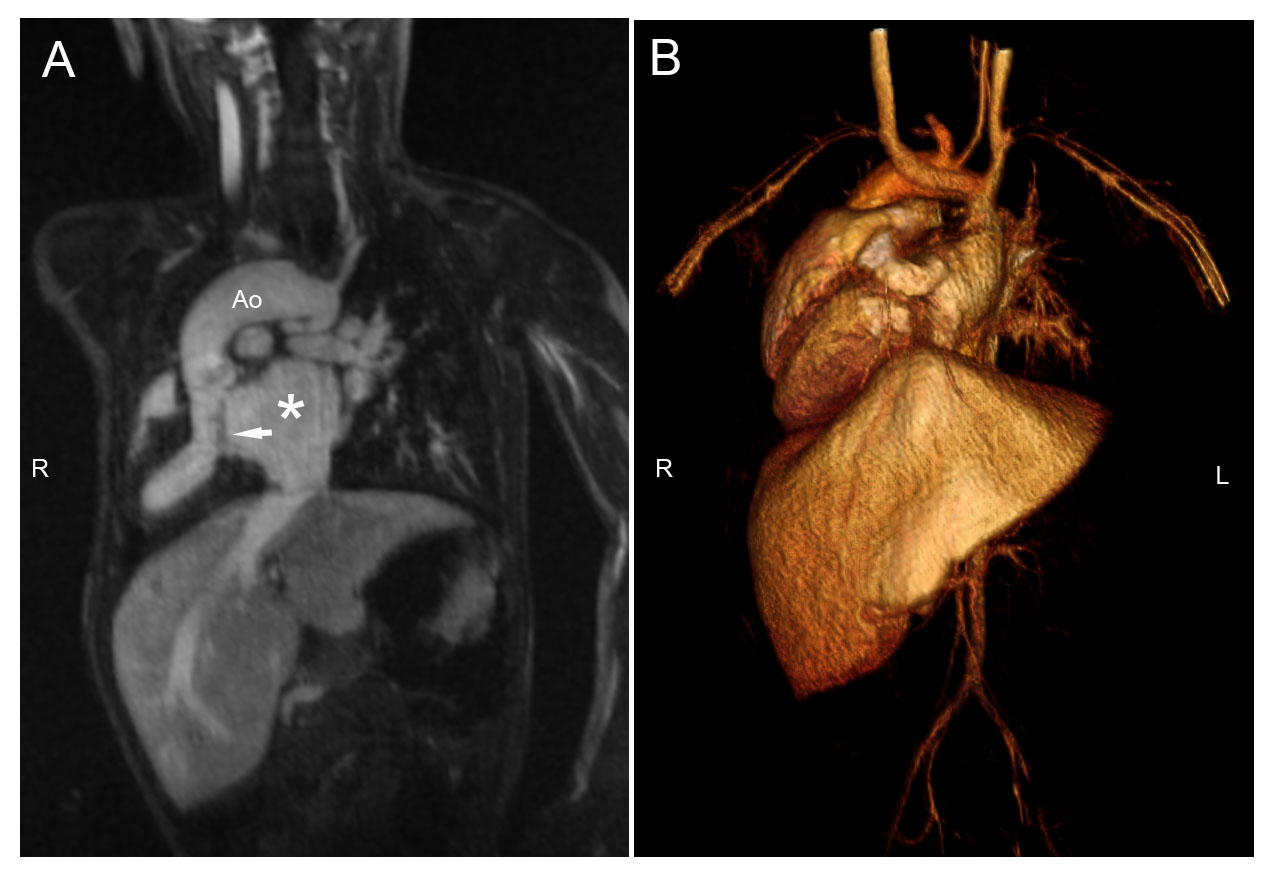
Between 2013-2017, a total of 129 patients with CHD underwent 4D-MUSIC (age range 1 day to 21 years, 51% male) across three U.S. medical centers. All cases were performed under controlled ventilation and general anesthesia. No ferumoxytol-related adverse events occurred. Ten patients had more than one 4D-MUSIC exam over 4 years. Four patients were classified as disease Group 1; the remaining patients belonged in Group 2 or 3. The predominant diagnoses were Tetralogy of Fallot and variants, double outlet ventricle, vascular rings /coarctation, and transposition of the great vessels. Creatinine ranged from 0.2 to 1.3 mg/dL. Image acquisition time for 4D-MUSIC ranged from 7-20 minutes depending on the number of cardiac phases; the total examination time (4D-MUSIC plus velocity mapping) ranged from 27-40 minutes. In all cases, 4D-MUSIC images were of diagnostic quality. The 3D isotropic resolution varied from 0.6-1.3mm and was dependent on patient size. Some older children had metallic implants with local signal loss (Figure 1), but overall image interpretation was not affected. In some very small children, lower signal-to-noise ratio was noted and streaking artifacts were observed at 1.5T and higher resolution (Figure 2), but the artifacts did not render the images non-diagnostic. In a small child with heterotaxy, complex intra-cardiac anatomy is well depicted (Figure 3). Images from all three sites, across a range of ages and intra-cardiac /vascular abnormalities were of comparable quality. A maximum value-added score of 5 was achieved for all exams across the three institutions.DISCUSSION:
FE 4D-MUSIC MRI provides value-added imaging in pediatric CHD. While recognizing that workflow efficiency may vary among institutions, implementation of FE 4D MUSIC across all three institutions was successful and early experience was highly reproducible across all sites. A combination of 4D-MUSIC with locally available phase contrast flow imaging was achievable in less than 40 minutes and sets a new standard for time efficiency and simplicity in CHD MRI. More widespread multi-center experience would be helpful for further validation of 4D-MUSIC.CONCLUSION:
Early experience with FE 4D-MUSIC for CHD imaging across three U.S. academic centers is promising. Highly reliable diagnostic images can be achieved and highly valued quality measures with respect to time efficiency, simplification of image acquisition, and alleviation of any concerns about Gd retention or renal function were reproducible.Acknowledgements
This work is supported by R01HL127153 from the National Heart, Lung, and Blood Institute.References
1. Han F, Rapacchi S, Khan S, Ayad I, Salusky I, Gabriel S, Plotnik A, Finn JP and Hu P. Four-dimensional, multiphase, steady-state imaging with contrast enhancement (MUSIC) in the heart: A feasibility study in children. Magnetic resonance in medicine : official journal of the Society of Magnetic. 2015 Oct;74:1042-1049
2. Han F, Zhou Z, Han E, Gao Y, Nguyen KL, Finn JP and Hu P. Self-gated 4D multiphase, steady-state imaging with contrast enhancement (MUSIC) using rotating cartesian K-space (ROCK): Validation in children with congenital heart disease. Magnetic resonance in medicine : official journal of the Society of Magnetic. 2017 Aug;78(2):472-483.
3. Finn JP, Nguyen KL and Hu P. Ferumoxytol vs. Gadolinium agents for contrast-enhanced MRI: Thoughts on evolving indications, risks, and benefits. J Magn Reson Imaging. 2017 Sep;46(3):919-923.
4. Bashir MR, Bhatti L, Marin D and Nelson RC. Emerging applications for ferumoxytol as a contrast agent in MRI. J Magn Reson Imaging. 2015 Apr;41:884-98.
5. Nguyen KL, Han F, Zhou Z, Brunengraber DZ, Ayad I, Levi DS, Satou GM, Reemtsen BL, Hu P and Finn JP. 4D MUSIC CMR: value-based imaging of neonates and infants with congenital heart disease. J Cardiovasc Magn Reson. 2017;19:40PMC5376692.
6. Everett AD. Cove Point Foundation: Helen B Taussig Children's Heart Center, Johns Hopkins University. Accessed November 6, 2017. http://www.pted.org/?id=overview1.
Figures