0913
Highly Accelerated Steady State Ferumoxytol Abdominal MRA using Compressed Sensing1Radiology, University of California, San Francisco, San Francisco, CA, United States, 2Siemens Healthcare, San Francisco, CA, United States, 3Siemens Healthcare, Erlangen, Germany
Synopsis
Clinical CE-MRA of the abdomen is limited in spatial resolution/coverage, or is excessively time consuming. We implemented a compressed sensing (CS) steady state MRA technique with an acceleration factor of 25, achievable in a 15 second breath hold, with 0.8mm isotropic resolution and a large 48cm coverage. In an investigation on 13 patients, we found CS-MRA had higher image quality scores and vessel sharpness compared with free breathing high-resolution MRA and clinical breath hold low-resolution MRA, with a reduced scan time. Our proposed CS-MRA technique is promising for the evaluation of abdominal vessels.
Introduction
Gadolinium based abdominal contrast enhanced MRA (CE-MRA) has been widely used in clinical practice to image a variety of abdominal vascular diseases, including aorto-iliac aneurysms and renal artery stenosis. Ultrasmall Superparamagnetic Iron Oxide (USPIO, Ferumoxytol) steady state MRA has been used as an alternative when the patient has poor renal function and cannot receive Gadolinium1. Despite the successes of these techniques, many technical challenges persist. Free breathing acquisitions necessitate a long scan time and may suffer from motion artifacts. Breath-hold acquisitions reduce motion artifacts, however, the reduced scan time (~25 seconds) results in limited coverage and lower resolution. Additionally, for some patients, a 25 second breath hold is not feasible. Novel acceleration techniques including compressed sensing (CS) have the potential to reduce scan time and increase spatial resolution while maintaining image quality 2, however validation in patients is still very limited. This study aims to develop a highly accelerated (a factor of 25), high resolution abdominal CS-MRA technique with initial validation in clinical patients.Methods
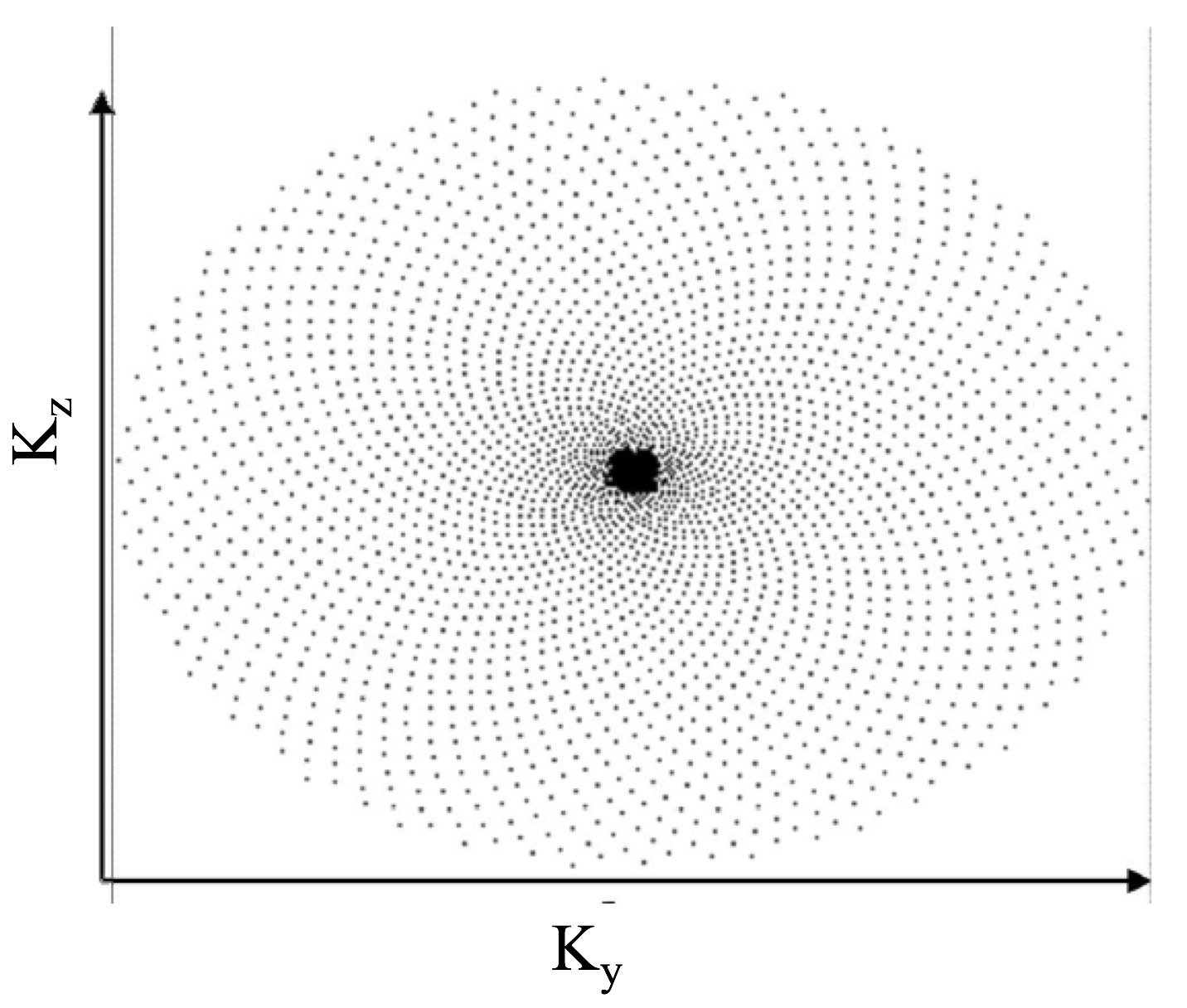
Study population: 13 patients with poor renal function or history of renal transplant (not eligible for Gadolinium contrast) and a variety of vascular diseases (abdominal aortic aneurysm, renal artery stenosis, or inflow peripheral vascular disease) were recruited. Ultrasmall Superparamagnetic Iron Oxide (USPIO) contrast agent (Ferumoxytol) was slowly infused into the patient before imaging. All scans were performed on a Siemens 3T system (MAGNETOM Skyra, Siemens Healthcare, Erlangen, Germany). Sequences: Three FLASH sequences were acquired: 1) Free breathing high-resolution MRA, 0.8mm isotropic resolution, 2 minutes scan time, 48cm FOV (head to foot direction). 2) Clinical breath-hold low-resolution MRA, 1.3-1.5mm isotropic, 25 second breath-hold, 36cm FOV. 3) Compressed sensing breath-hold high-resolution MRA used a prototype sequence previously implemented 2, 0.8mm isotropic, 15 second breath-hold, 48cm FOV. For the CS-MRA, the k-space data were acquired using a highly under-sampled (R=25) Cartesian spiral phyllotaxis sampling pattern (Figure 1) and reconstructed directly on the scanner with an iterative SENSE technique (L1 regularized in the wavelet domain). A regularization factor of 0.002 and 20 iterations were used. The online reconstruction took 5 minutes in the background. Image Analysis: Two radiologists scored images (1-5 scale) of the large vessels (aorta/iliacs) and renal arteries, and measured the aortic diameter. Lumen to muscle contrast ratio, lumen signal inhomogeneity (SD/mean), and sharpness were quantified and compared. Paired one-way ANOVA was used to compare the three techniques.Results
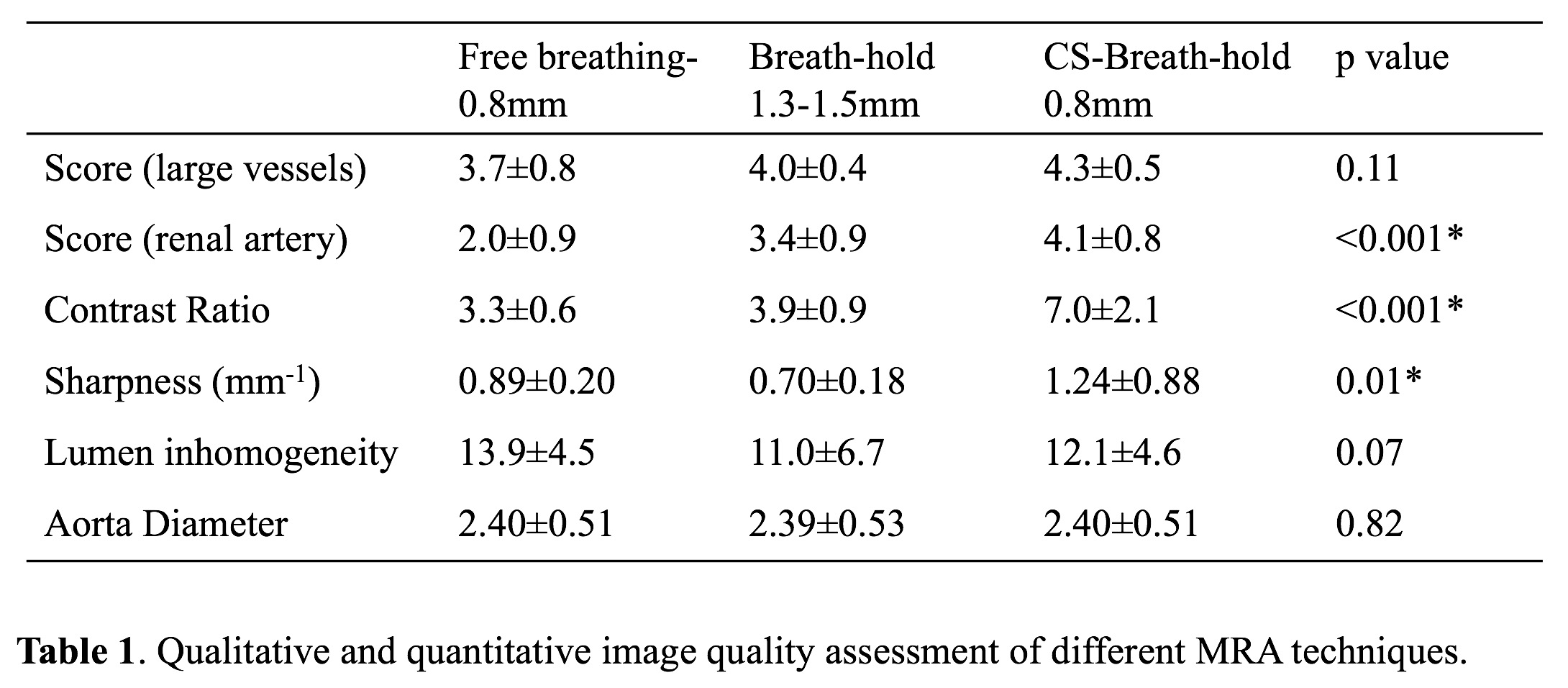
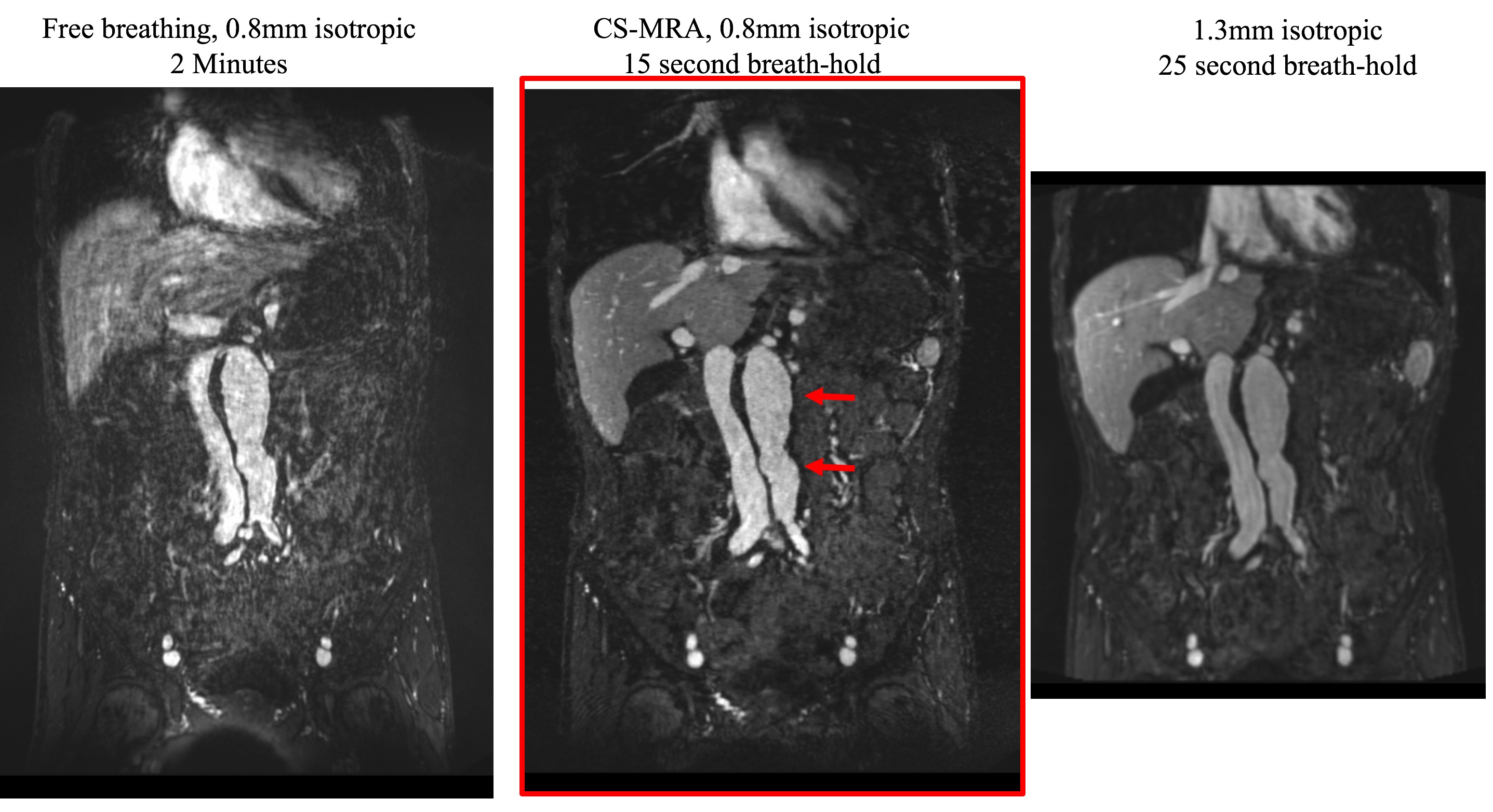
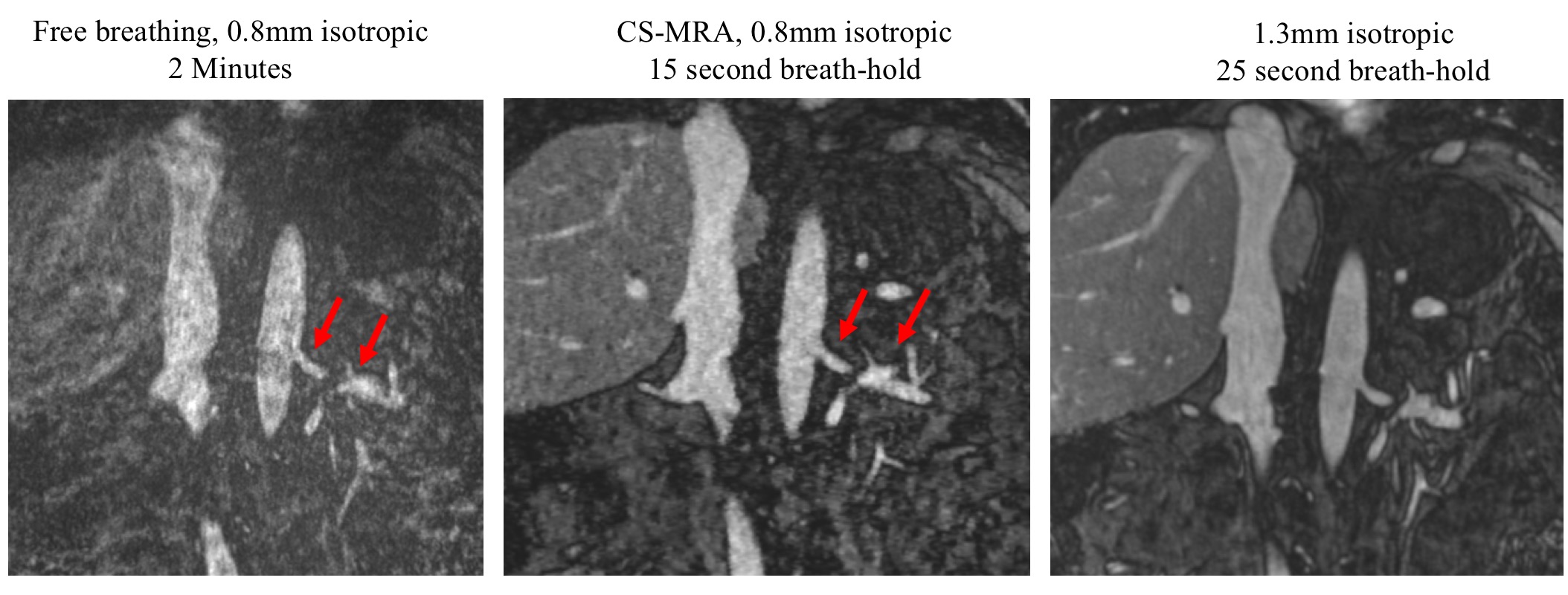
Two radiologists had good agreement for image scoring and diameter measurements (ICC = 0.73 and 0.99), and a qualitative and quantitative image quality matrix for the 3 sequences is shown in Table 1. All three sequences achieved good and comparable image quality for large vessels (average scores >3.8, p=0.11). Delineation of the renal arteries was significantly improved with the breath-hold techniques compared to the free-breathing acquisition, with CS-MRA achieving the best image quality. All three techniques had comparable lumen inhomogeneity, and aortic diameter measurements showed no dependence on acquisition. CS-MRA had the highest contrast ratio and lumen sharpness. Sample images of an abdominal aortic aneurysm are shown in Figure 2, and images of the renal arteries are shown in Figure 3. Free breathing MRA commonly suffered from breathing artifacts. Low-resolution breath-hold MRA had limited coverage and the lowest sharpness (resolution). Breath-hold CS-MRA had the best image quality, highest sharpness, and the shortest scan time.Discussion
To our knowledge, this is the first study validating compressed sensing methods for breath hold abdominal contrast enhanced MRA. We achieved good image quality with a factor of 25 acceleration, making 0.8mm isotropic resolution (1/5 voxel size of clinical breath hold MRA) and a large coverage of 48cm realizable in a 15 second breath hold. While low resolution breath hold MRA was sufficient for the evaluation of large vessels, the higher resolution of CS-MRA significantly increased the image sharpness, improving the evaluation of smaller vessels like the renal and superior mesenteric arteries. The shorter breath-hold (15 seconds vs. 25 seconds for clinical CE-MRA) improves patient comfort and reduces the likelihood of a nondiagnostic exam. Although a steady state contrast agent was used in this study, allowing for repeat imaging and thus balanced evaluation of the 3 contrast-enhanced acquisitions, the CS-MRA technique developed here can be used for first-pass Gadolinium MRA without modification. Future work is need to evaluate its feasibility for first-pass Gadolinium MRA.Conclusion
Highly accelerated compressed sensing contrast-enhanced MRA is a promising tool for the evaluation of abdominal vessels with high resolution, large coverage, and short scan time.Acknowledgements
No acknowledgement found.References
1. Hope MD, Hope TA, Zhu C, Faraji F, Haraldsson H, Ordovas KG, et al. Vascular imaging with ferumoxytol as a contrast agent. AJR. American journal of roentgenology. 2015;205:W366-373
2. Stalder AF, Schmidt M, Quick HH, Schlamann M, Maderwald S, Schmitt P, et al. Highly undersampled contrast-enhanced mra with iterative reconstruction: Integration in a clinical setting. Magnetic resonance in medicine. 2015;74:1652-1660
Figures