0866
Impaired cerebrovascular reactivity assessed by BOLD hypercapnic fMRI is associated with increased risk of stroke in patients with symptomatic intracranial atherosclerotic stenosis1Department of Neurology, University Hospital Grenoble Alpes, Grenoble, France, 2Neuroradiology, University Hospital of Grenoble Alpes, Grenoble, France, 3Univ. Grenoble Alpes, Inserm, Grenoble Institute of Neurosciences, Grenoble, France, 4Univ. Grenoble Alpes, Inserm, CNRS, University Hospital Grenoble Alpes, IRMaGe, Grenoble, France
Synopsis
Intracranial atherosclerotic stenosis (IAS) remains at risk of recurrent ischemic events despite intensive medical management. Cerebrovascular reactivity (CVR) assessed by hypercapnic challenge using BOLD functional MRI (CVR BOLD fMRI) estimates cerebrovascular reserve and may allow to identify patients at higher risk of recurrent ischemic events. 19 patients referred for unilateral symptomatic IAS were studied to estimate the relationships between baseline characteristics, recurrence of ischemic events, and CVR. During follow-up, recurrent ischemic events were more frequent in patients with impaired CVR. CVR mapping may help to better select among IAS patients those at higher risk to discuss additional treatment.
Introduction
In patients with symptomatic intracranial atherosclerotic stenosis, recurrent ischemic events occur despite optimal medical therapy1. Additional treatments such as endovascular angioplasty and stenting are still not validated. Indeed, large trials failed to demonstrate significant clinical benefits when compared to higher risks of mordibity and mortality2. To further address additional therapy, the estimation of cerebrovascular reserve may help to better identify patients at higher risk of stroke recurrence. Cerebrovascular reactivity assessed by hypercapnic challenge using BOLD functional MRI (CVR BOLD fMRI) has been proposed to estimate cerebrovascular reserve and to identify patients at higher risk3. We studied the relationships between baseline characteristics of patients with unilateral symptomatic IAS, recurrence of ischemic events, and CVR BOLD fMRI.
Patients and Methods
Nineteen patients with symptomatic unilateral IAS of middle cerebral artery (MCA) or internal carotid artery were selected (61.0±12.5yo). We performed fMRI of perfusion to measure basal perfusion using DSC, and CVR elicited by hypercapnic challenge (8%CO2) using BOLD contrast (32 slices, voxel=4x4x4mm, TR/TE/α=3000/35ms/90°, 240 dynamics in 12min during a block-design hypercapnic stimulus; 3T AchievaTX, Philips). Individual end-tidal CO2 pressure (mmHg) was simultaneously recorded and further used as a physiological regressor to conduct linear regression analysis. Post-processing was performed using AMIGOv0.9, an in-house software (Python3.6, Matlab8.6, SPM12), giving whole-brain and regional basal CBF, CBV, MTT, and CVR. We calculated statistical relationships between individual clinical and biological baseline characteristics, recurrent ischemic events, basal perfusion, and CVR BOLD fMRI in MCA territories (CVRMCA) reported using laterality indices (LI) for each parameter, with LI=(Left-Right)/(Left+Right). Normal |LI CVRMCA| was <0.08, as previously defined in healthy volunteers4.Results
During follow-up (mean±SD=3.57±1.43 years), we identified 2 groups: 12 patients had a single ischemic qualifying event (SINGLE), and 7 patients experienced at least a recurrent ipsilateral ischemic event (RECURRENT). Overall annual risk of recurrent ipsilateral ischemic event was 18.4% per year.
Comparisons between SINGLE and RECURRENT groups
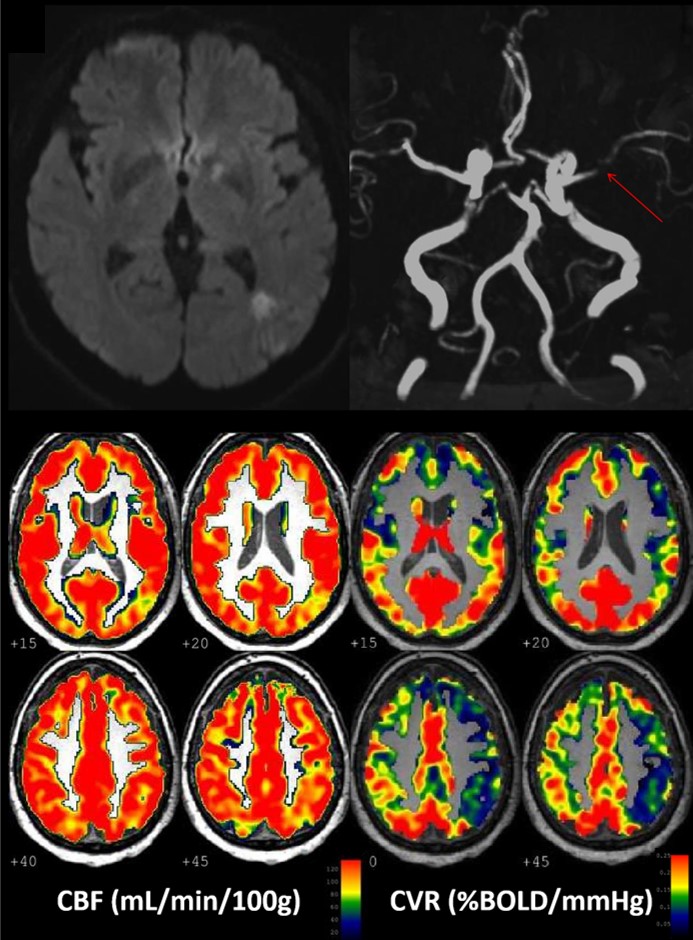
When compared with SINGLE, RECURRENT patients were older (69.5±9.1. vs 56.1±11.8 p=0.04). There were no differences among other clinical and biological data. RECURRENT patients had higher |LI| CVRMCA (0.14±0.05 vs 0.05±0.03, p=0.001). There were no differences among |LI| CVR in other arterial territories. Subtle intergroup differences in basal perfusion parameters did not reach significance. Illustrative cases are shown in Figures 1 and 2.
Comparisons between IMPAIRED and NORMAL CVRMCA groups
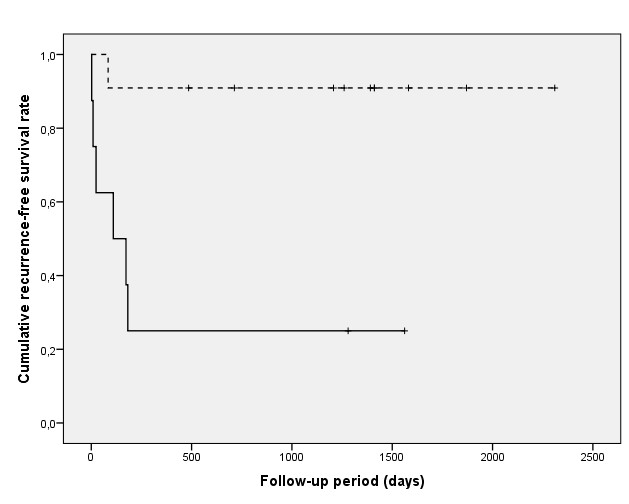
Among all patients, 11 patients had NORMAL CVRMCA, and 8 had IMPAIRED CVRMCA. There were no intergroup differences among clinical and biological baseline data. The occurrence of recurrent ipsilateral ischemic event in IMPAIRED CVRMCA (n=6/8) was more frequent than in NORMAL CVRMCA group (n=1/11) with different survival curves (p=0.003) (Figure 3). The annual risk of recurrent ipsilateral ischemic event was higher in IMPAIRED CVRMCA group compared to NORMAL CVRMCA group (39.1%/year vs 3.4%/year, p=0.012). There were neither differences among |LI| CVR in other arterial territories nor in other basal perfusion parameters.
Conclusion
Impaired CVR assessed by BOLD hypercapnic fMRI is associated with higher risk of stroke in patients with symptomatic IAS. CVR mapping should be considered to identify among IAS patients those at a higher risk of recurrent ischemic event and to select those who may benefit from additional treatment, such as endovascular procedures.
Acknowledgements
No acknowledgement found.References
1. Mazighi, M. et al. Prospective study of symptomatic atherothrombotic intracranial stenoses: the GESICA study. Neurology 2006;66:1187–1191
2. Chimowitz, M. I. et al. Stenting versus Aggressive Medical Therapy for Intracranial Arterial Stenosis. N. Engl. J. Med. 2011;365:993–1003
3. Smeeing, D. P. J., Hendrikse, J., Petersen, E. T., Donahue, M. J. & de Vis, J. B. Arterial Spin Labeling and Blood Oxygen Level-Dependent MRI Cerebrovascular Reactivity in Cerebrovascular Disease: A Systematic Review and Meta-Analysis. Cerebrovasc. Dis. Basel Switz. 2016;42:288–307
4. Boudiaf, N. et al. BOLD fMRI of cerebrovascular reactivity in the middle cerebral artery territory: A 100 volunteers’ study. J. Neuroradiol. 2015;42:338–344
Figures
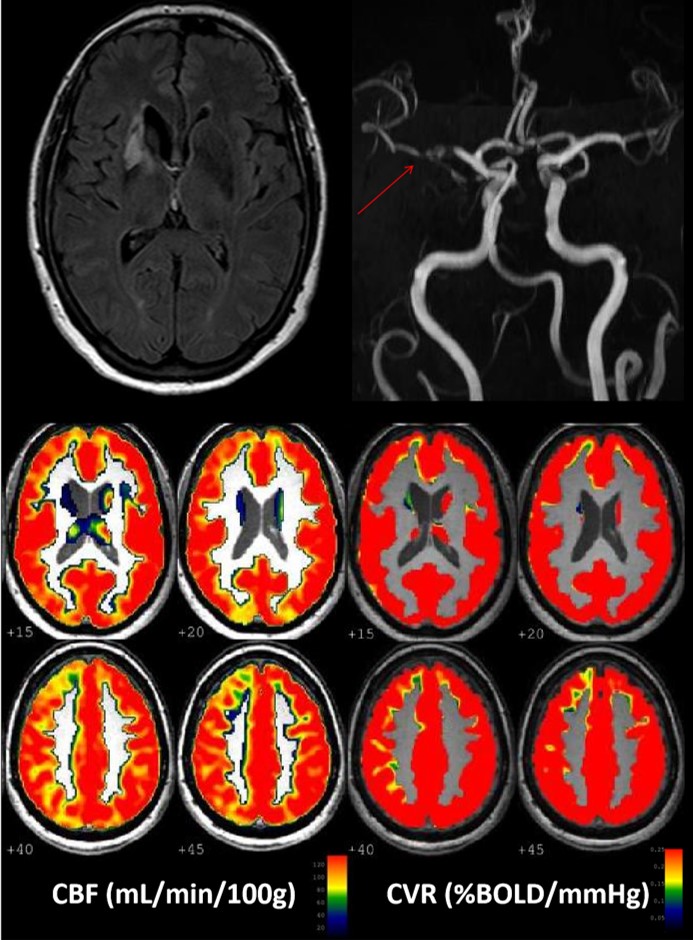
Illustrative case of 62yo female, referred of a symtpomatic left MCA stenosis (arrow). CBF was symmetrical with |LI|CBFMCA=0.02, while CVR was impaired downstream IAS with |LI|CVRMCA=0.12. Transient ischemic attacks occured twice during follow-up despite aggresive medical treatment.
B = femme de 62 ans, sténose M1 gauche (85%), 2 récidives AIT. Valeurs de CBF, CBV, MTT symétriques, CVR diminuée en aval de la sténose (|LI|CBFACM=0.02,|LI|CVRACM = 0.12).