0864
Intravoxel Incoherent Motion (IVIM) Perfusion Imaging in Hyperacute Stroke: Initial Results1University Hospital Basel, Basel, Switzerland, 2Neuroradiology, Stanford University, Stanford, CA, United States, 3Neurology, Stanford University, Stanford, CA, United States
Synopsis
Intravoxel Incoherent Motion (IVIM) MR perfusion is of particular interest in stroke because it derives intrinsic microvascular perfusion information, and might therefore include information regarding collateral blood flow without being influenced by time delay in blood arrival, which is a limitation of other perfusion techniques. In this preliminary work in 23 patients with hyperacute stroke, we found the IVIM microvascular perfusion paramteters were significantly reduced in the infarct core but not in the penumbra, compared to the contralateral side, suggesting that at time of imaging, microvascular perfusion is maintained through collateral blood flow in the penumbra.
INTRODUCTION
The Intravoxel Incoherent Motion (IVIM) MR perfusion method is be of particular interest in stroke, because it derives intrinsic microvascular perfusion information from a multi-b value diffusion-weighted sequence, and therefore, might include information regarding collateral blood flow without being influenced by time delay in blood arrival. Consequently, IVIM might be able to determine the quality of the collateral blood flow in the ischemic (or at risk of becoming ischemic), but viable, penumbra. The IVIM perfusion method has been validated in a variety of paradigms.1 In 3 studies in human acute stroke,2,3,4 the IVIM perfusion parameter f was shown to be reduced on average in the infarcted area, but those studies were performed outside the therapeutic window. The aim of this work was to study the IVIM perfusion parameters in the hyperacute stroke, in both the infarct core and the penumbra.METHODS
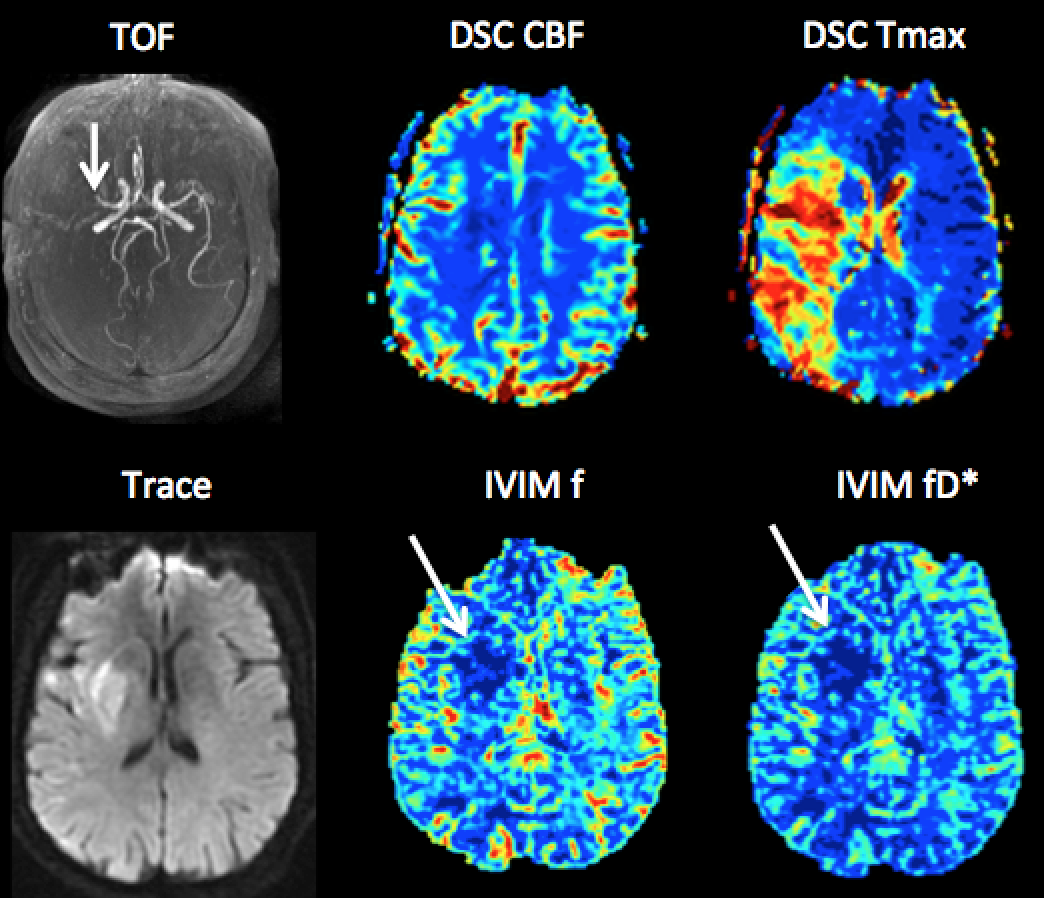
Patients undergoing triage for endovascular acute stroke treatment were included, with confirmed supratentorial stroke on MRI and imaging performed <16 hours of last seen well. A short multiple b-values diffusion-weighted MRI sequence, using a monopolar pulsed gradient scheme and a spin-echo planar imaging (EPI) readout, was added the standard hyper-acute stroke protocol, with following acquisition parameters: 6 b-values (1000, 200, 150, 100, 50, 0) in three orthogonal directions, TR/TE, 4200/78 ms; FOV 249×240 mm2; slice thickness, 5 mm; acquisition matrix, 128 × 128; in-plane physical resolution of 1.9 × 1.9 mm2; parallel imaging accelerating factor 2; 75% Fourier encoding; receiver bandwidth 1953 Hz/pixel. Post-processing: The trace was computed for each b-value. The IVIM bi-exponential signal equation model was fitted using a C++ implementation of a standard two-step algorithm, where in the first step D was fitted using a mono-exponential signal equation on values b > 200 s/mm2, and in the second step, during which D, as acquired in the first step was kept fixed, the IVIM bi-exponential signal equation was fitted on all b-values using the Levenberg-Marquardt algorithm. Quantitative analysis: Regions of interest were drawn in the infarct core (defined as D < 600mm2/s), in the corersponding region in the contralateral hemisphere, and in the penumbra, defined using dynamic susceptibility contrast perfusion imaging Tmax imaging (Tmax >6s). The IVIM perfusion parameters were assessed by averaging the trace for each b-value in the region of interest before the fitting. Statistical analysis: Statistical significance was tested using Wilcoxon-Test. Significance level was set to α < 0.05.RESULTS
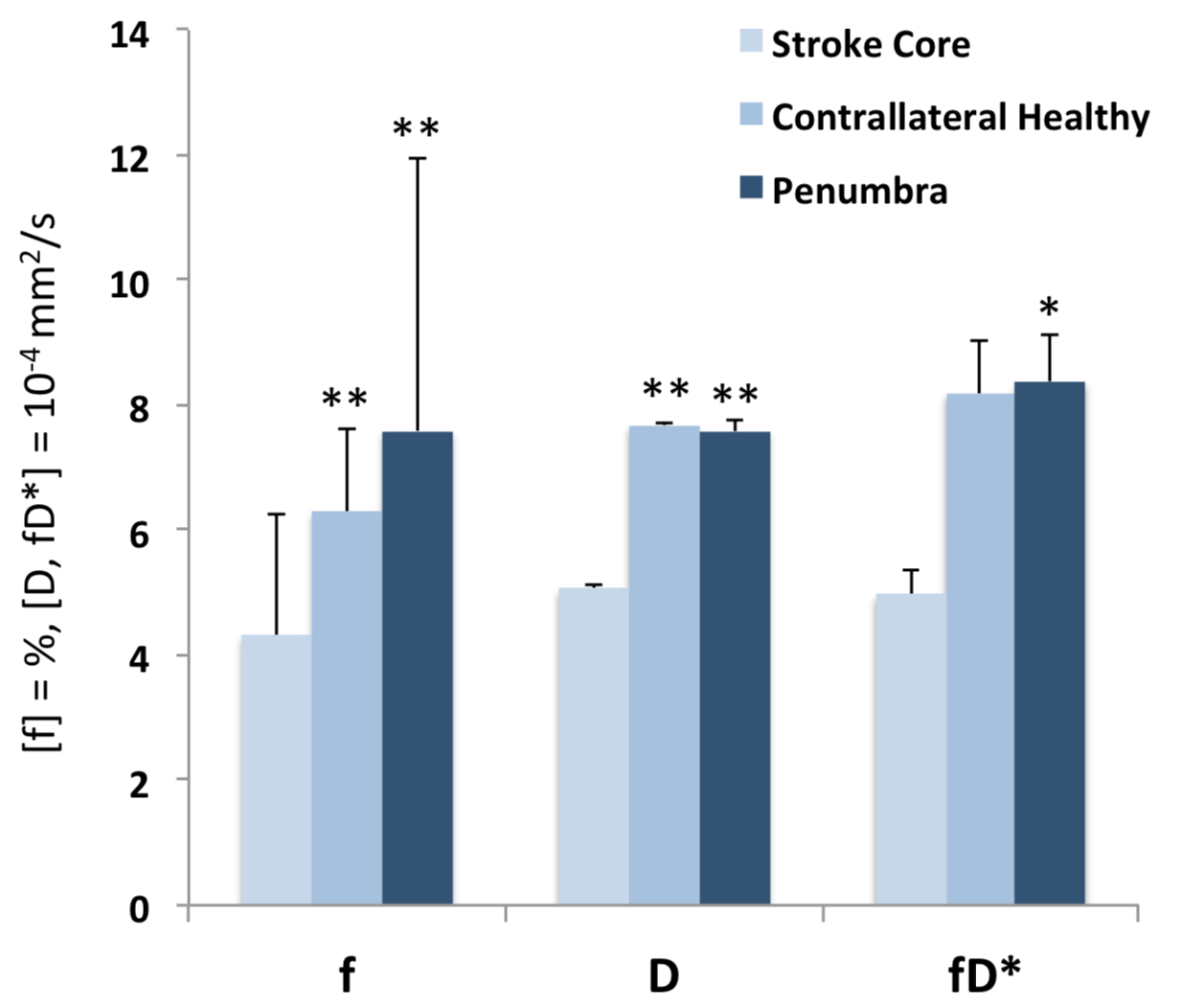
23 patients (male/female=11/12, mean age 69.6±12.5y) were included. Mean infarct core volume was 44±61 ml, mean penumbra volume was 86±83 ml, and mean time from symptom onset to imaging was 344±144 min. In the stroke core, IVIM f was significantly lower ([mean ± standard deviation] 4.3±1.9% compared to the healthy contralateral region (6.3±1.3%, p<0.001), as well as compared to the penumbra (7.5±4.3%; p<0.002). IVIM fD* was reduced significantly in the stroke core (5.0±4.0 10-4 mm2/s) compared to the penumbra (8.0±6.4 10-4 mm2/s, p<0.003). No significant difference was found for both IVIM f and fD* between penumbra and the healthy contralateral region (p=0.09 and p=0.46 respectively). As expected, D was significantly reduced in the stroke core (5.0±0.1 10-4 mm2/s) compared to both the contralateral region (7.7±0.0 10-4 mm2/s, p<0.001) and the penumbra (7.6±0.2 10-4 mm2/s, p<0.001), while no significant difference in D was found between contralateral region and the penumbra (p=0.4).DISCUSSION
In our preliminary results, in accordance with the published literature at later time point after stroke onset2,3,4, we found that IVIM microvascular perfusion is significantly reduced in the infarct core in the hyperacute stroke compared to the contralateral side as well as compared to the penumbra. In addition, we found that IVIM microvascular perfusion in the penumbra is retained, suggesting that at time of imaging, microvascular perfusion is maintained through collateral blood flow in the penumbra. Therefore, IVIM perfusion imaging might be a marker of the quality of the collateral blood flow in the penumbra in hyperacute stroke patients.Acknowledgements
Christian Federau is supported by the Swiss National Science Foundation
References
1. Federau C. Intravoxel incoherent motion MRI as a means to measure in vivo perfusion: A review of the evidence, NMR in Biomed. 2017 Nov;30(11). doi: 10.1002/nbm.3780
2. Federau C et al. Intravoxel incoherent motion perfusion imaging in acute stroke: initial clinical experience. Neuroradiology. 2014;56(8):629‐635.
3. Yao Y et al. Intravoxel incoherent motion diffusion‐weighted imaging in stroke patients: initial clinical experience. Clin Radiol. 2016;71(9):938 e911‐938 e936.
4. Suo S et al. Stroke assessment with intravoxel incoherent motion diffusion‐weighted MRI. NMR Biomed. 2016;29(3):320‐328.
Figures