0824
T1 Mapping and MR Elastography (MRE) for the Diagnosis of Mild Chronic Pancreatitis1Shengjing Hospital of China Medical University, Shen Yang, China, 2Philips Healthcare, Beijing, China
Synopsis
We have investigated the value of both MR elastography (MRE) and T1 mapping for early detection of Mild Chronic pancreatitis(CP). Our study found that both MRE and T1 mapping had good diagnostic performance for detecting mild CP, with MRE slightly outperforming T1 mapping.
Introduction
CP is a progressive disease of inflammation and fibrosis that may cause severe intractable pain and endocrine insufficiency 1. The diagnosis of CP is usually inferred from the results of conventional imaging modalities. Previous study reported that the T1 relaxation time of the pancreas increased in mild CP patients when compared with healthy pancreas2. However, no MRE study has been conducted in diagnosing mild CP. Hence, the purpose of this study was to determine whether the pancreatic stiffness determined by MRE and T1 relaxation time of the pancreas determined by T1 mapping could be used for evaluation of mild CP.Methods
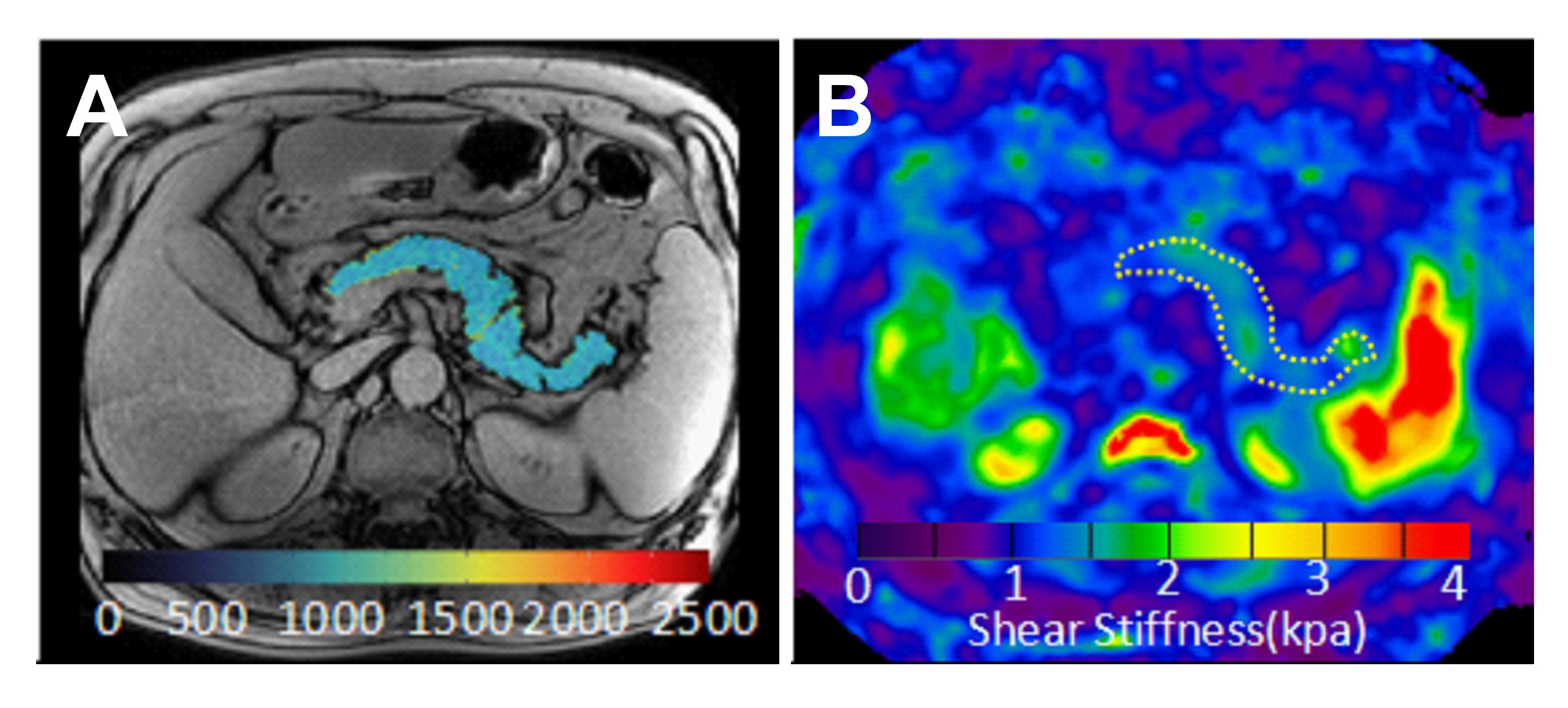
This Institutional Review Board (IRB)-approved, Health Insurance Portability and Accountability Act (HIPAA)-compliant retrospective study analyzed 48 patients with suspected mild CP. Patients were grouped as normal (n=23) or mild CP (n=25) according to the Cambridge classification based on history, presenting symptomatology, and concordant findings on endoscopic retrograde cholangiopan-creatography (ERCP)1. All subjects underwent both T1 mapping (Philips 3.0T Ingenia, Philips Healthcare, the Netherlands) and MRE (Signa HDX system; GE Healthcare, Milwaukee, WI). MRE using a multislice echo planar imaging (EPI) sequence with an automated three-dimensional (3D) wave field inversion algorithm was used to generate pancreatic stiffness maps. The imaging parameters were set up as following: frequency=40Hz; TR/TE = 1375ms/38.8ms; phase offsets = 3; FOV = 40 cm; acquisition matrix = 96×96; number of signal averages = 1; frequency-encoding direction = RL; parallel imaging acceleration factor = 3; number of slices = 32; slice thickness = 3.5 mm. The imaging parameters for T1 mapping was as follows: TR/TE= 2.24ms/1.01ms; FOV=30cm; acquisition matrix = 152×150; slice thickness = 10mm; breathhold duration=12 sec; flip angle of 20; acquisition matrix =152 x 150; NSA= 1. Diagnostic accuracy and area under the curve (AUC) of both MRE and T1 mapping was calculated by using receiver operating characteristic (ROC) analysis.Results
The pancreatic stiffness of mild CP was 1.53±0.14kPa, significantly higher than that of those without mild CP (1.20±0.13kPa, P<0.01). MRE (pancreatic stiffness >1.35kPa) showed significantly better diagnostic performance for detecting mild CP than that achieved by T1 mapping (T1 relaxation time>878.4msec) (AUC: 0.963 vs 0.850, P=0.043). Although MRE showed slightly improved sensitivity (88% vs 84%, P=1.000), specificity (95.7% vs 82.6%, P=0.375) and accuracy (91.7% vs 83.3%, P=0.344), none of these comparisons reached statistical significance.Conclusion
Both MR elastography and T1 mapping had good diagnostic performance for detecting mild CP, with MRE slightly outperforming T1 mapping.Discussion
The T1 mapping technique was an accurate method for detecting CP 2, directly measuring the T1 relaxation time of the pancreas. Theoretically, the T1 relaxation time is tissue-specific and independent of imaging parameters and with minimal variances using different vendors 3. As proven in our study, MRE was slightly better than T1 relaxation times for detecting mild CP. MRE measures the mechanical properties quantitatively and reflects both fibrosis and inflammation 4. Theoretically, MRE is also interchangeable across MRI machines and strength magnet. As long as it is performed at the same frequency, the stiffness should remain unchanged. Both MRE and T1 mapping are fast and simple MRI techniques, without contrast media, showing promising techniques to diagnose mild CP.Acknowledgements
We thank Richard Ehman and Kevin Glaser from the Mayo Clinic for providing the MRE system. We also thank Jun Chen from the Mayo Clinic for his assistance with providing the tailored pancreatic MRE driver. This work was supported by a grant from the National Natural Science Foundation of China (No. 81771893, 81771802 and NIH EB1801).References
1.Conwell D L, Lee L S, Yadav D, et al. American Pancreatic Association practice guidelines in chronic pancreatitis: evidence-based report on diagnostic guidelines. Pancreas.2014;43(8):1143-1162.
2.Tirkes T, Chen L, Fogel E L, et al. T1 Mapping for Diagnosis of Mild Chronic Pancreatitis. Journal of Magnetic Resonance Imaging Jmri. 2017; 45(4):1171-1176.
3.Schelbert E B, Messroghli D R. State of the Art: Clinical Applications of Cardiac T1 Mapping. Radiology.2016;278(3):658.
4.Shi Y, Guo Q, Xia F, et al. MR Elastography for the Assessment of Hepatic Fibrosis in Patients with Chronic Hepatitis B Infection: Does Histologic Necroinflammation Influence the Measurement of Hepatic Stiffness? Radiology.2014;273(1):88-98.
Figures