0760
Feasibility of Free-Breathing Fetal Cine Cardiac MRI based on Doppler Ultrasound, Compressed Sensing and Motion Compensation1Lund University, Skåne University Hospital, Department of Clinical Sciences Lund, Clinical Physiology, Lund, Sweden, 2Laboratory of Computing, Medical Informatics and Biomedical-Imaging Technologies, School of Medicine, Aristotle University, Thessaloniki, Greece, 3Lund University, Skåne University Hospital, Department of Clinical Sciences Lund, Diagnostic Radiology, Lund, Sweden, 4Department of Diagnostic and Interventional Radiology, University Medical Center Hamburg-Eppendorf, Hamburg, Germany, 5North medical GmbHMartinistraße 52, 20246, Hamburg, Germany, 6Faculty of Engineering, Lund University, Department of Biomedical Engineering, Lund, Sweden, 7Siemens Healthcare AB, Malmö, Sweden, 8Lund University, Department of Health Sciences, Physiotherapy, Lund, Sweden
Synopsis
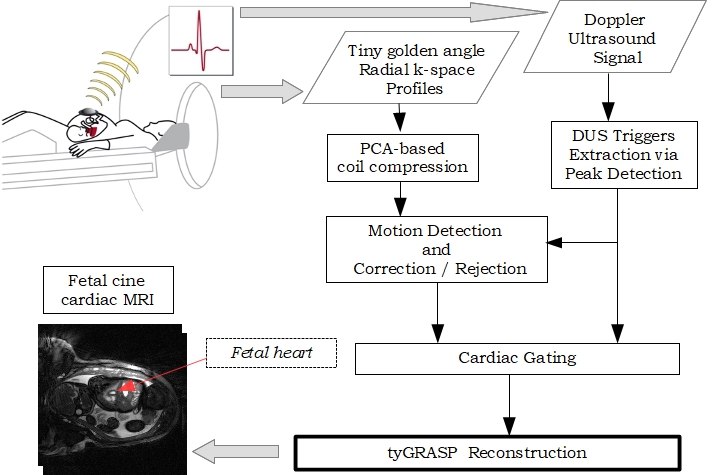
We investigated the feasibility of free-breathing fetal cine cardiac MRI using Doppler Ultrasound retrospective binning combined with continuous tiny golden angle radial sampling and compressed sensing via the tyGRASP reconstruction method. Motion due to maternal respiration and fetal movement was estimated by registration applied to reconstructed images of low temporal resolution. K-space radial profiles containing motion were either corrected or rejected from the reconstruction process. The reconstruction results demonstrated good image and diagnostic quality showing that the absence of fetal ECG can be bypassed in a computationally efficient way by Doppler Ultrasound even in the presence of motion.
Background
Fetal cardiac MRI is a viable tool for evaluating the fetal heart both for research and clinically. The extraction of a reliable fetal ECG is an open problem due to low voltages, contamination by the maternal ECG, and MRI-related interference. Solutions based on retrospectively sorting the acquired data into the proper cardiac phases have been proposed and applied using standard pulse sequences1,2. The aim of this study was to demonstrate the feasibility of free-breathing fetal cine CMR using Doppler Ultrasound-gated retrospective binning combined with continuous tiny golden angle radial sampling and compressed sensing tyGRASP (tiny Golden-angle RAdial Sparse Parallel)3,4. Motion due to maternal respiration and fetal movement is estimated and the corresponding k-space profiles are either corrected or rejected from the reconstruction process.Methods
Regional Review Board approval and written informed consent from the study participants were obtained. Exams were performed on a 1.5T MAGNETOM Aera system (Siemens Healthcare GmbH, Erlangen, Germany).
A flowchart of the proposed reconstruction method is shown in Figure 1. Short-axis and four-chamber view human fetal cardiac data were acquired using a radial trajectory with a constant azimuthal increment of tiny golden angle of order seven4 corresponding to 23.63o with a prototype balanced Steady State Free Precession sequence with the following parameters: TE/TR=1.88/3.7ms, flip angle 60ο, pixel size 0.7x0.7x4 mm3. A total of 13 short-axis and 6 four-chamber slices with 4,000 radial spokes-per-slice were acquired during maternal free breathing in two fetuses at gestational week 35. The cardiac synchronization signal required for the binning stage was produced by a prototype MRI-compatible Doppler Ultrasound (DUS) device (sMaRT-sync, north medical Gmbh, Germany)5. The DUS synchronization signals were determined using raw Doppler signals and processed using software written in MATLAB (The MathWorks, Natick, MA, USA). The number of cardiac phases depended on the number of available cardiac cycles, with typical values ranging between 16 to 22 phases. Motion due to maternal respiration and fetal movement was detected using translational registration applied to an image series with low temporal resolution: for each cardiac cycle, only one image was reconstructed using the corresponding radial profiles which were available via the DUS synchronization signal. As expected, the motion of the pulsating fetal heart was smoothed out, and therefore, any displacements depicted in these images were due to maternal respiration and fetal movement. When the detected movement was approximately translational, it was corrected by the appropriate shift operation in k-space. Otherwise, the corresponding profiles were not used for the reconstruction. The final images were obtained by using the tyGRASP method3. The reconstruction time was approximately 5 minutes-per-slice on a standard computer. An observer with 17 years of cardiovascular MRI experience scored image quality and cardiac/extracardiac diagnostic quality on 4-grade scales where intrauterine image quality 1=low quality and/or high degree of artifact; 2=moderate quality and/or some artifacts; 3=high quality and/or few artifacts; and 4=high quality; and diagnostic quality 1=inadequate; 2=low; 3=moderate; 4=high. Cardiac diagnostic quality was based on discernible epi- and endocardial borders to surrounding tissue and blood pool, visualized papillary muscles/trabeculation, potential of measurement of wall thickness, visualized wall thickening during contraction, and potential detection of ventricular septal defects or other cardiac pathology; and extracardiac diagnostic quality was based on thoracic structures outside the heart, brain structures, contrast between brain and cerebrospinal fluid, spinal cord visualization, abdominal structures, and placental structure and attachment. Scores are presented as median (range).
Results
Intrauterine image quality, cardiac and extracardiac diagnostic quality were 2 (2-3), 3 (3-4) and 3 (3-4), respectively. In Figure 2, the sixteen reconstructed cardiac phases of two different slices of a short-axis view are shown cropped and magnified. In these slices, no translational motion was identified and therefore, their reconstruction was based on the k-space profiles left after the rejection of the ones containing movement. Figure 3 shows an indicative translational motion correction result of a four-chamber view slice. The reconstructed images without motion correction are blurred and the boundaries of the anatomical structures are less clear. The improvement in sharpness after motion correction is evident. These initial results on two subjects (four multi-slice datasets, 36 free-breathing slices in total) verified qualitatively that the DUS-based gating signal is accurate even in the presence of shallow motion, and therefore, it can be used for the cardiac binning stage.Conclusions
This study demonstrates that free-breathing Doppler Ultrasound-gated fetal cardiac cine MRI based on tyGRASP is possible with good image and diagnostic quality. Maternal respiratory motion and fetal movement were detected via registration in low-temporal DUS-based reconstructions, and compensated for. In the future, these methods can be tuned and automated thus minimizing user interaction and further promoting the use of fetal cardiovascular imaging clinically.Acknowledgements
Funding was provided by the Swedish Heart and Lung Foundation, the Skåne University Hospital and by the Medical Faculty at Lund University. The authors thank and acknowledge Siemens Healthcare for providing support within the Master Research Agreement with Lund University and the Region of Skåne.References
- Jansz MS et al MRM 64:1304 (2010)
- Haris K et al JMRI 46:207 (2017)
- Feng L et al MRM 72:707 (2014)
- Wundrak S et al IEEE TMI 34:1262 (2015)
- Kording F et al MRM 74:1257 (2015)
Figures