0759
Clinical value of dark-blood late gadolinium enhancement without additional magnetization preparation1Department of Radiology, Maastricht University Medical Centre, Maastricht, Netherlands, 2School of Biomedical Engineering and Imaging Sciences, King's College London, London, United Kingdom, 3Department of Cardiology, St Thomas' Hospital, London, United Kingdom, 4Department of Cardiology, Antwerp University Hospital, Antwerp, Belgium, 5British Heart Foundation Centre of Excellence, King's College London, London, United Kingdom, 6Pontificia Universidad Católica de Chile, Escuela de Ingeniería, Santiago, Chile
Synopsis
Late gadolinium enhancement (LGE) MRI often suffers from poor scar-to-blood contrast when used for detection of (sub)endocardial scar due to the bright signal of adjacent blood. We sought to validate a novel dark-blood LGE technique in a large cohort of 250 patients at both 1.5T and 3T. Combining left ventricular blood nulling with phase-sensitive inversion-recovery significantly improved both image quality and diagnostic confidence compared to conventional bright-blood LGE. As no additional magnetization preparation is used,
Background
Late gadolinium enhancement (LGE) has been the reference standard in the assessment of myocardial viability for almost two decades now. Although its ability to depict myocardial infarction from viable myocardium is well known, the bright signal of adjacent blood may reduce, or even completely obscure, areas of thin subendocardial scarring. In addition, the left ventricular (LV) blood signal can even mimic scar tissue and lead to false positive observations. Simply shortening the inversion time to null the LV blood magnetization not only results in a negative signal of the viable myocardium, which appears equally as bright as scar due to the magnitude image reconstruction, but also leads to significantly smaller scar size [1,2]. Numerous methods have been proposed to reduce LV blood signal using various additional magnetization preparation schemes, including T2 preparation, magnetization transfer, T1 rho using spin locking, and double and triple inversion recovery [3-7]. However, most of these schemes are not readily available or require extensive optimizations, software modifications, and/or additional training.
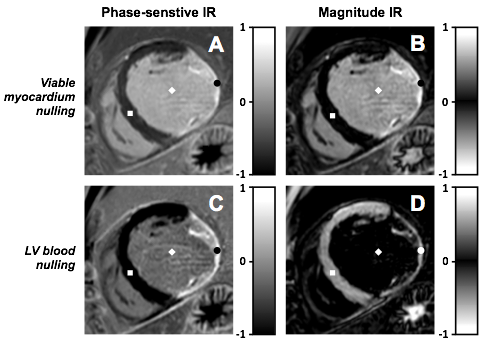
Recently, a novel method was developed that significantly reduces LV blood signal, without using additional magnetization preparation, and evaluated in nine patients with ischaemic scar on a 1.5T scanner [8]. This method combines the use of phase-sensitive inversion recovery (PSIR) and nulling LV blood magnetization instead of viable myocardium magnetization. PSIR’s ability to distinguish between positive and negative longitudinal magnetization provides an opportunity to achieve a darker LV blood signal whilst preserving bright scar and dark viable myocardium signal. Setting a shorter inversion time, such that the LV blood magnetization is at the null point of recovery, leads to a darker-gray appearance of LV blood in the PSIR image (figure 1). The negative magnetization from viable myocardium, that would appear bright in a magnitude image, now appears completely black, as PSIR reveals its negative phase. The positive scar magnetization still appears bright due to its fast recovery, leading to an increased dynamic contrast range and therefore offering excellent contrast between areas of (subendocardial) scar and both LV blood and viable myocardium. We sought to validate this novel dark-blood LGE technique in a large cohort of patients at both 1.5T and 3T.
Methods
250 consecutive patients referred for a clinical cardiac MRI exam were enrolled and randomly allocated to three different scanners (Philips Ingenia 1.5T: n=86, Philips Achieva 3T: n=79 and Siemens Aera 1.5T: n=85). A routine cardiac MRI protocol was performed using both functional cine and LGE imaging. An intravenous injection of 0.2 mmol/kg gadobutrol (Gadovist; Bayer, Germany) was administered prior to LGE imaging. Ten minutes after contrast agent injection, PSIR LGE imaging was performed twice using different inversion times to acquire a full stack of short axis images with conventional viable myocardium nulling and one with LV blood nulling. A Look-Locker scan (TI scout) was performed before each stack to determine the optimal inversion time for the required tissue nulling. All images were acquired during 10–15 s breath-holds. The presence and pattern of scar, global image quality, and diagnostic confidence were assessed for both methods by five independent readers who were blinded to clinical data and image type. Definite diagnosis of ischaemic or non-ischaemic scar was made by expert consensus.Results
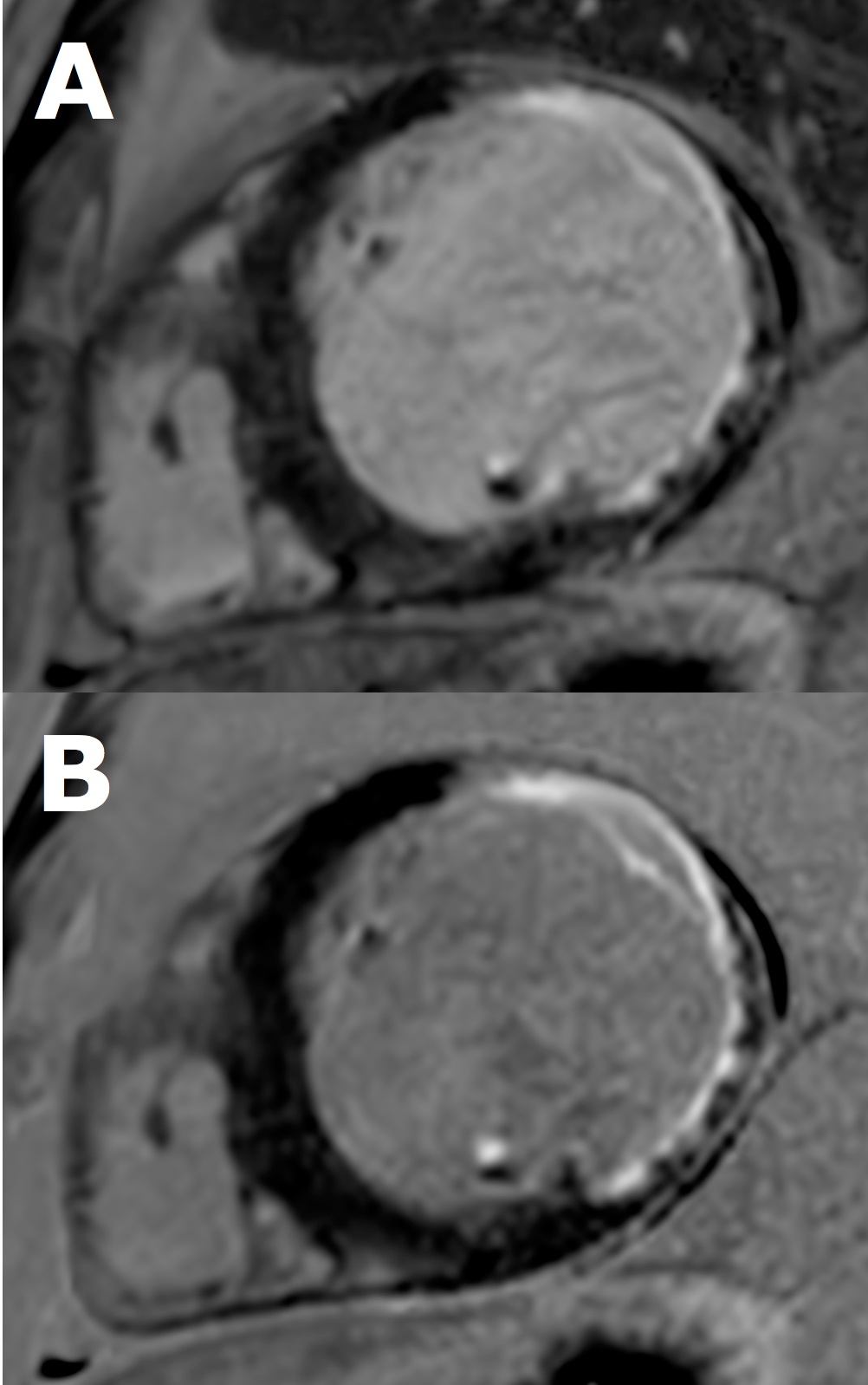
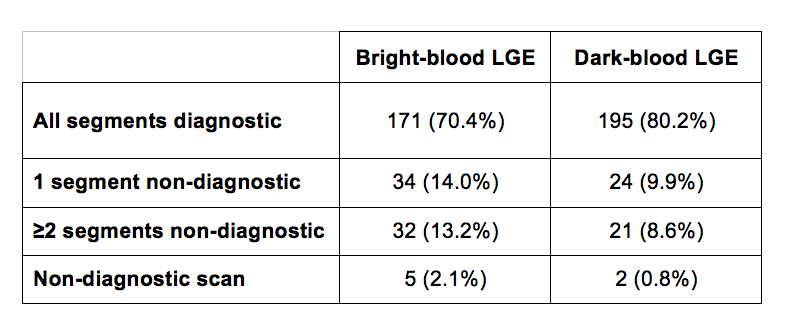
Complete bright-blood and dark-blood PSIR LGE data sets were available in 243 patients (figure 2). All patients with a definite diagnosis of ischaemic scar (n=57) were identified using dark-blood LGE, while only 53 patients were identified using conventional bright-blood LGE. Global image quality was significantly higher when using dark-blood LGE compared to bright-blood LGE (p=0.001): All LV segments were diagnostic in 80.2% and 70.4% of all patients, respectively (table 1). Diagnostic confidence did significantly improve when using dark-blood LGE compared to bright-blood LGE (81.1% vs 70.7%, p=0.001). No significant differences between 1.5T and 3T were observed.Discussion
Dark-blood PSIR LGE imaging is a feasible, readily available MR method to detect myocardial scar with improved image quality and diagnostic confidence compared to conventional bright-blood LGE imaging, on both 1.5 and 3T. Nulling LV blood magnetization for PSIR LGE allows visualization of contrast-enhanced tissues, while supressing the LV blood signal, and thereby improving subendocardial scar conspicuity. Improved scar conspicuity was confirmed by the fact that all ischaemic scar patients were successfully identified using dark-blood LGE, while four of those patients (7% of total) were missed using conventional bright-blood LGE, and therefore potentially misdiagnosed. As no additional magnetization preparation is required for this novel method, clinical application on current MR systems is readily available without the need for extensive optimizations, software modifications, and/or additional training.Acknowledgements
NoneReferences
1. Kellman P, Arai AE, McVeigh ER, et al. Phase-sensitive inversion recovery for detecting myocardial infarction using gadolinium-delayed hyperenhancement. Magn Reson Med. 2002;47(2):372–83.
2. Setser RM, Chung YC, Weaver JA, et al. Effect of inversion time on delayed-enhancement magnetic resonance imaging with and without phase-sensitive reconstruction. J Magn Reson Imaging. 2005;21(5):650–5.
3. Kellman P, Olivieri L, Grant E, et al. Dark blood late gadolinium enhancement improves conspicuity of ablation lesions. J Cardiovasc Magn Reson 2016;18(1):P211.
4. Kim HW, Rehwald WG, Wendell DC, et al. Flow-independent dark-blood DeLayed enhancement (FIDDLE): validation of a novel black blood technique for the diagnosis of myocardial infarction. J Cardiovasc Magn Reson. 2016;18(1):O55.
5. Liu C-Y, Wieben O, Brittain JH, et al. Improved delayed enhanced myocardial imaging with T2-prep inversion recovery magnetization preparation. J Magn Reson Imaging. 2008;28(5):1280–6.
6. Muscogiuri G, Rehwald WG, Schoepf UJ, et al. T (rho) and magnetization transfer and INvErsion recovery (TRAMINER)- prepared imaging: a novel contrast-enhanced flow-independent dark-blood technique for the evaluation of myocardial late gadolinium enhancement in patients with myocardial infarction. J Magn Reson Imaging. 2016;30:1–9.
7. Peel SA, Morton G, Chiribiri A, et al. Dual inversion-recovery MR imaging sequence for reduced blood signal on late gadolinium-enhanced images of myocardial scar. Radiology. 2012;264(1): 242–9.
8. Holtackers RJ, Chiribiri A, Schneider T, et al. Dark-blood late gadolinium enhancement without additional magnetization preparation. J Cardiovasc Magn Reson. 2017;19(1):64
Figures