0718
Measurement using 3D-FSE-T2WI is useful in predicting early recovery of continence following radical prostatectomy in patients with prostate carcinoma.Tatsuya Shimizu1, Utaroh Motosugi1, Satoshi Funayama1, Takahiko Mitsui2, Masayuki Takeda2, and Hiroshi Onishi1
1Radiology, University of Yamanashi Hospital, Chuo-shi, Japan, 2Urology, University of Yamanashi Hospital, Chuo-shi, Japan
Synopsis
We conducted a prospective study to examine if preoperative anatomical evaluation of the urethra using 3D-FSE-T2WI is useful in predicting early recovery of continence following total prostatectomy in patients with prostate carcinoma. The length of the membranous urethra (8.4±1.7 mm vs. 5.7±0.6 mm, p=0.005) and the thickness of the pelvic diaphragm (10.8±1.4 mm vs. 8.8±0.5 mm, p=0.01) were significantly different between the patients who achieved continence and those who did not achieve continence 1 month after surgery. A longer membranous urethra and thicker pelvic diaphragm measured using 3D-FSE-T2WI are correlated to earlier recovery of continence following radical prostatectomy.
Introduction
Radical prostatectomy is a conventional definitive treatment option for localized prostate cancer, and urinary incontinence is one of the major complications after prostatectomy. The time taken to achieve stable urinary continence after prostatectomy varies among patients. Several previous studies have shown that anatomical variations in the urethra can be the cause of the variation1,2. Therefore, we conducted a prospective study to examine if preoperative anatomical evaluation of the urethra using three-dimensional fast spin echo T2-weighted imaging (3D-FSE-T2WI) is useful in predicting early recovery of continence following total prostatectomy in patients with prostate carcinoma.Methods
Between May 2015 and May 2017, 27 patients with newly diagnosed prostate cancer were enrolled. All patients underwent pre-operative magnetic resonance (MR) imaging including 3D-FSE-T2WI on a 3-T MR system: TR=3000 ms, TE=90 ms, ETL=40, and voxel size=0.8 × 1.0 × 2.0 mm. A radiologist measured the following anatomical features on the MR images using original and reformatted images: length of the membranous urethra, thickness of the pelvic diaphragm and levator ani, and the volume of the prostate gland. The length of the membranous urethra and thickness of the pelvic diaphragm were measured using sagittal images. The levator ani thickness was measured from the maximal length converging on the urethra on an axial image immediately caudal on the prostate apex. The volume of the prostate was calculated using the ellipsoid volume formula. We measured the maximum anterior–posterior, lateral, and vertical diameters of the prostate on the MR images and substituted those values into the formula. A urologist evaluated the voiding symptoms at 1 and 3 months after surgery at an outpatient clinic. Incontinence was defined using the International Consultation on Incontinence Questionnaire – Short Form (ICIQ-SF) and number of urine pads used per day. The student’s t-test was used to compare MR imaging parameters between the continent and incontinent groups. Data analysis was performed using JMP version 11 (SAS Institute Japan, Tokyo, Japan). Results with p-values less than 0.05 were considered statistically significant.Result
Recovery of continence was achieved in 11.1% (3/27) and 38.5% (10/27) of the patients at 1 and 3 months after surgery, respectively. The length of the membranous urethra (8.4±1.7 mm vs. 5.7±0.6 mm, p=0.005) and the thickness of the pelvic diaphragm (10.8±1.4 mm vs. 8.8±0.5 mm, p=0.01) were significantly different between the patients who achieved continence and those who did not achieve continence 1 month after surgery. However, no significant difference was observed 3 months after the surgery (p=0.06 and p=0.97, respectively). The thickness of the levator ani and the volume of the prostate were not related to recovery of continence after surgery (p=0.38 and p=0.27, respectively). Regarding the surgical procedure, 23 patients underwent robot-assisted laparoscopic radical prostatectomy, and 4 patients underwent radical retropubic prostatectomy. Urinary continence rates after surgery were not significantly different between the two groups.Discussion
After radical removal of prostate gland, distal sphincteric unit seem to have significant role to achieve early recovery of urinary continence.Conclusion
A longer membranous urethra and thicker pelvic diaphragm measured using 3D-FSE-T2WI are correlated to earlier recovery of continence following radical prostatectomy.Acknowledgements
No acknowledgement found.References
1. Coakley FV, Eberhardt S, Kattan MV, et al. Urinary continence after radical retropubic prostatectomy: relationship with membranous urethral length on preoperative endorectal megnetic resonance imaging. J Urol. 2002; Sep;168(3):1032-5.
2. Song C, Doo CK, Hong DH, et al. Relationship between the integrity of the pelvic floor muscles and early recovery of continence after radical prostatectomy. J Urol. 2007 Jul;178(1):208-11.
Figures
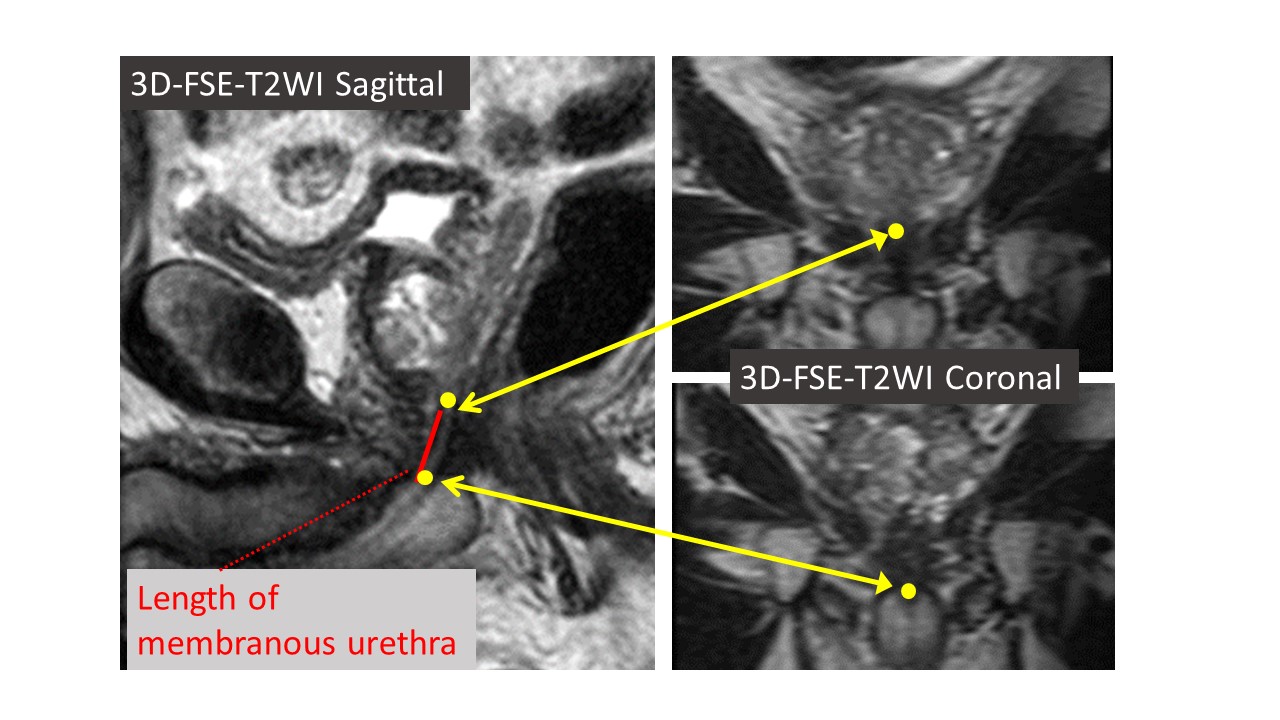
Measurement of membranous urethra
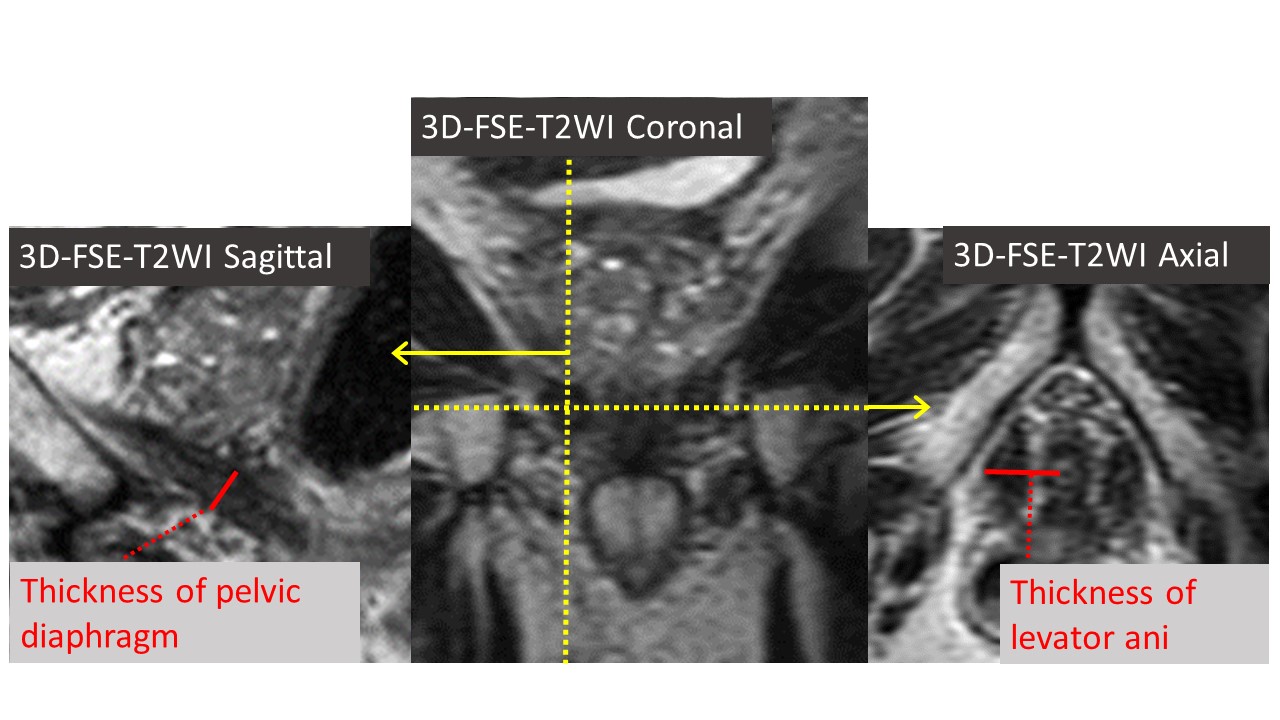
Measurement of pelvic diaphragm and levator ani
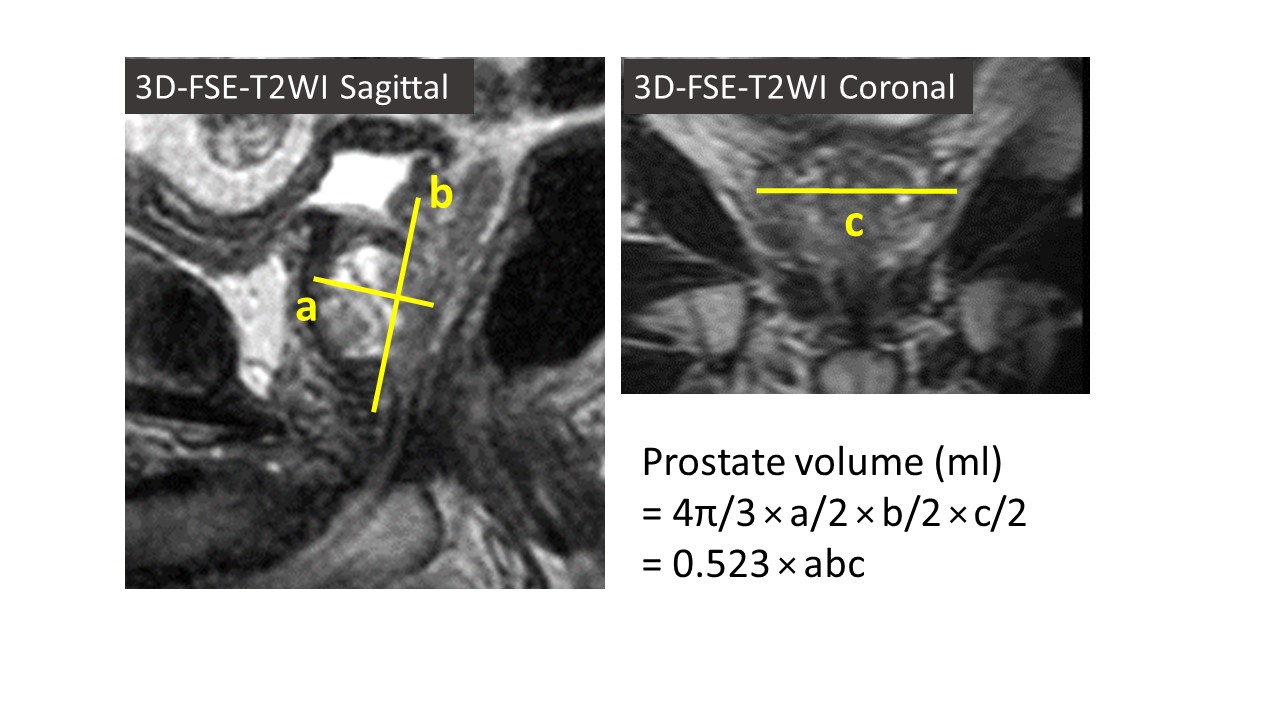
Calculation method of prostatic volume
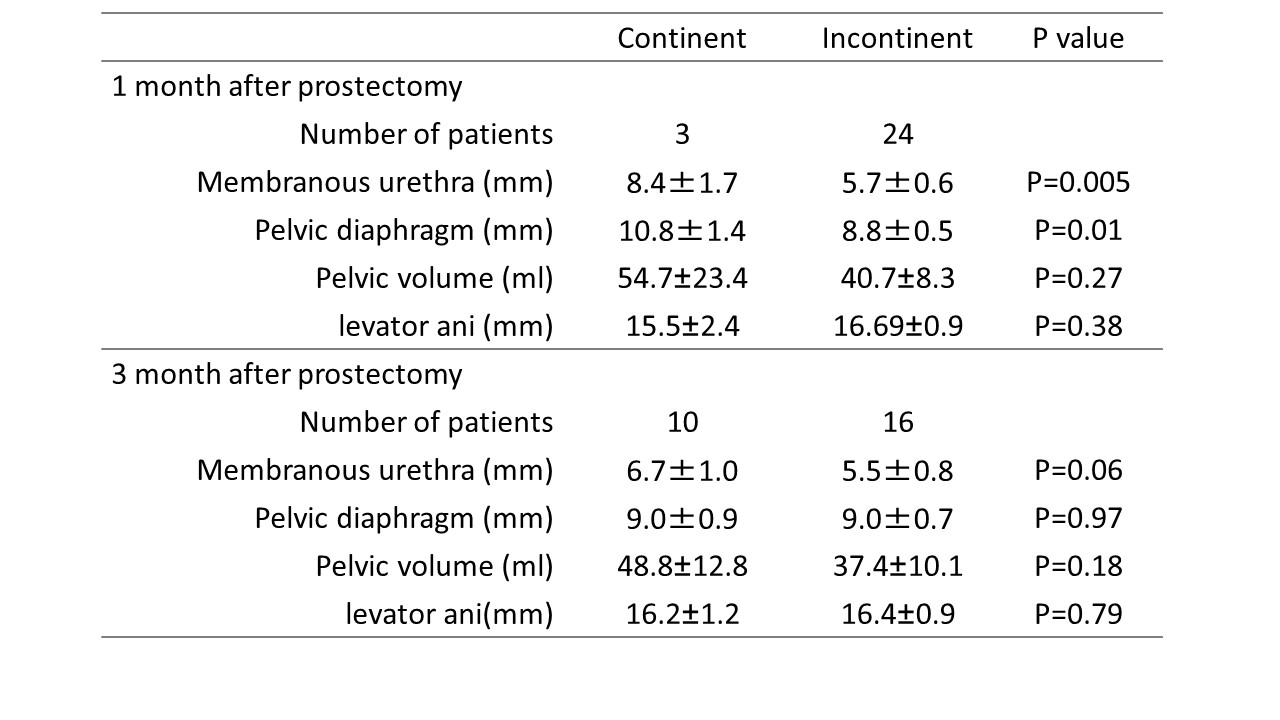
Result
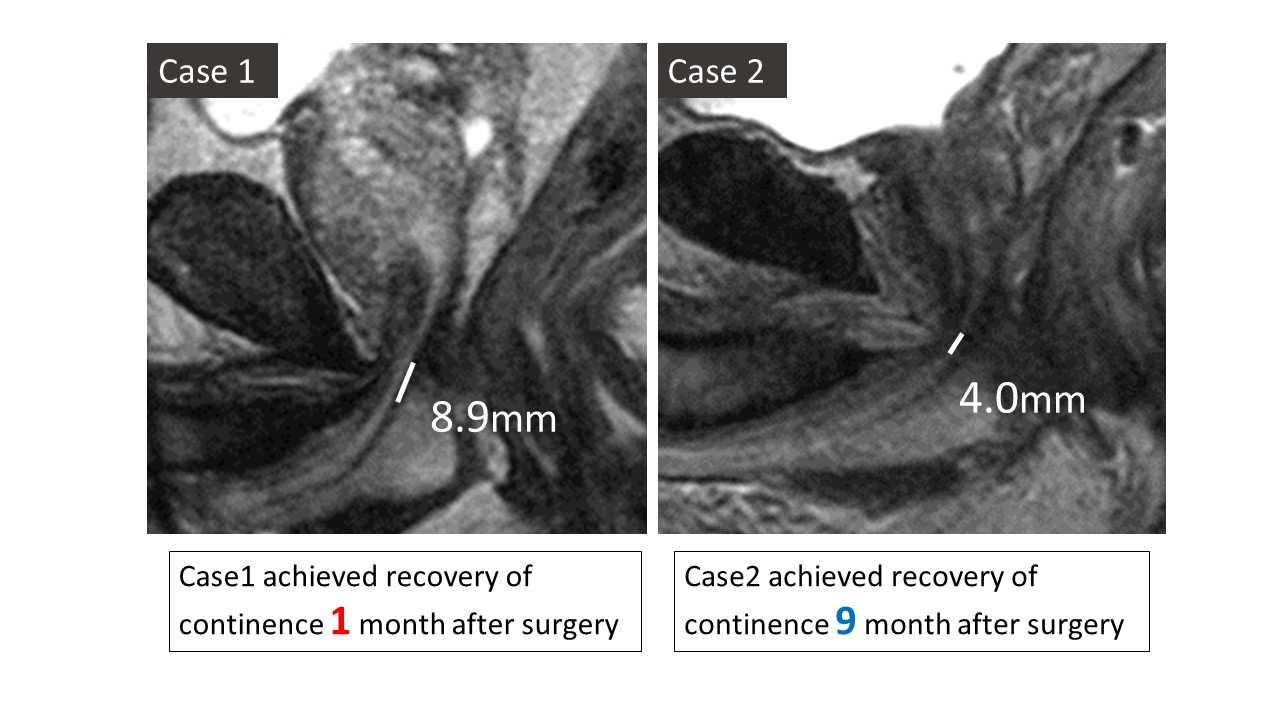
Case presentation