0699
A novel strategy for automated near-real-time segmentation of the ventral-intermediate (VIM) nucleus for deep brain stimulation (DBS) surgery1Electrical and Computer Engineering, University of Arizona, Tucson, AZ, United States, 2Surgery, University of Arizona, Tucson, AZ, United States, 3Medical Imaging, University of Arizona, Tucson, AZ, United States
Synopsis
Direct visualization of thalamic nuclei using MRI has been challenging for applications such as Deep Brain Stimulation (DBS) surgery for treatment of essential tremor, where the ventral intermediate (VIM) nucleus is targeted. Current methods are mainly based on Diffusion Tensor Imaging (DTI) which is limited by low spatial resolution and distortion of EPI as well as manual post processing such as seeding specific areas to identify the cerebro thalamic tract. We have developed a novel strategy that combines a white-matter nulled MPRAGE sequence followed by fast near-real time automated segmentation of thalamic nuclei, which can be tailored for each patient for accurate targeting of the VIM nucleus.
Introduction
Essential tremor can effectively be treated with DBS electrode implantation in the ventral-intermediate (VIM) nucleus of the thalamus. It is a complex procedure, usually performed using frame stereotaxis and pre-operative MRI/CT along with electrophysiological track exploration whilst the patient is awake. Asleep DBS is more suitable for anxious or dystonic patients but requires precise localization and, ideally, direct targeting of the VIM nucleus on MRI scans. The thalamic nuclei are often invisible in conventional anatomical MRI. Diffusion-tensor based methods have shown promise especially those involving the cerebro-thalamic tract (CTT). However, these are limited by poor spatial resolution and distortion of echo-planar imaging (EPI). Recently, a white-matter nulled (WMN) magnetization-prepared rapid gradient-echo (MPRAGE) sequence1 in combination with automated thalamic nuclei segmentation2 was successfully used for fast segmentation of thalamic nuclei. We adapted this methodology to investigate near-real-time segmentation of the VIM nucleus for asleep DBS.Methods
Segmentation of pre-operative MRI data
We used Shortened Template and Thalamus for Optimal Multi Atlas Segmentation (ST THOMAS)2 for segmentation of the VIM nucleus on pre-operative WMN-MPRAGE data. It uses 20 WMN atlases with manual segmentations to segment the thalamic nuclei from WMN-MPRAGE data in under 15 minutes on a dual-CPU 4-core 3GHz Intel Xeon Dell workstation. Briefly, the input image is cropped and nonlinearly registered to each of the 20 cropped atlas images and the resulting 20 labels combined using a joint fusion algorithm that assigns weights based on image similarity.
Evaluation of accuracy on patients with traditional DBS surgery
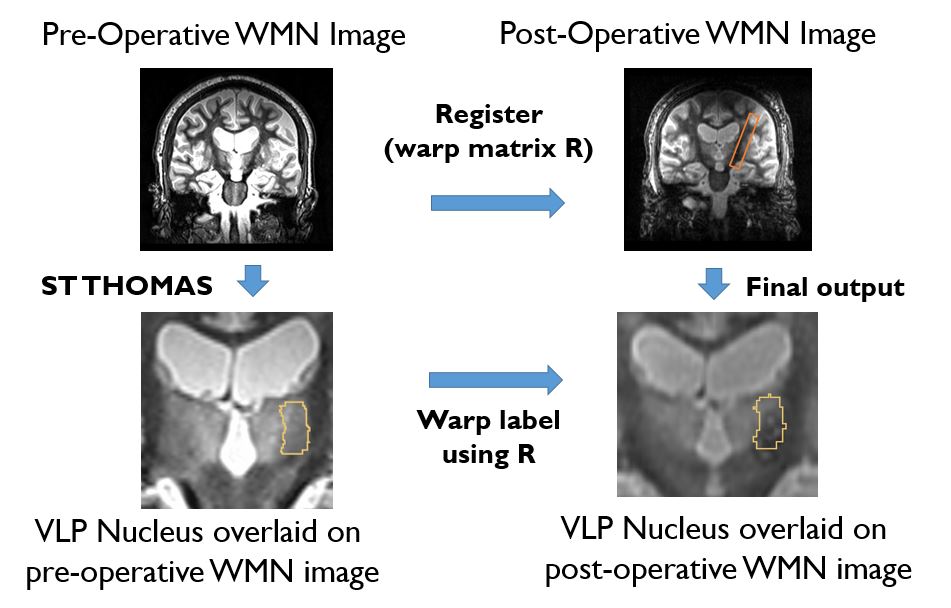
To evaluate the accuracy of our strategy, the VIM nucleus segmented from the pre-operative WMN-MPRAGE data using ST-THOMAS was warped to and then overlaid on post-operative WMN-MPRAGE images to visualize the location of the electrode tip relative to the VIM nucleus. This was done on four patients who had pre-operative MRI on a Siemens 3T MRI scanner and then underwent traditional awake DBS implantation. Both linear affine and non-linear registration, with and without masking were performed using Advanced Normalization Tools (ANTs). The mask was obtained by manually segmenting the metal electrode artifact (signal dephasing) on a slice-by-slice basis in post-operative WMN-MPRAGE. This is illustrated in Figure 1. This procedure takes less than 10 minutes, ideal for real-time awake DBS .
Validation on patients with asleep DBS surgery
We evaluated our strategy on patients undergoing asleep DBS surgery on a 1.5T GE MRI scanner using a Clearpoint navigation system (MRI Interventions, Irvine, CA) with traditional atlas-based targeting of VIM nucleus. On these patients, both intra-operative and post-operative WMN MPRAGE were available, the former being desirable due to lack of metal artifacts.
MRI acquisition
All patients were scanned pre-operatively on a 3T Siemens MRI scanner (Skyra) and post/intra-operatively on a 1.5T GE MRI Scanner (Signa HDx) after informed consent following institutional review board guidelines. In addition to the standard sequences, a WMN-MPRAGE was also acquired on all scans. Scan parameters were similar to traditional 1mm isotropic resolution MPRAGE except TI was chosen to null WMN (~500ms at 3T). A radial view ordering was used to minimize motion.
Results
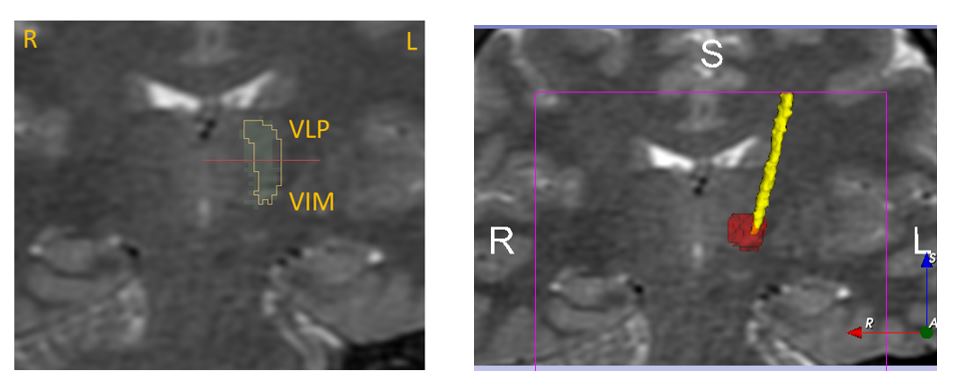
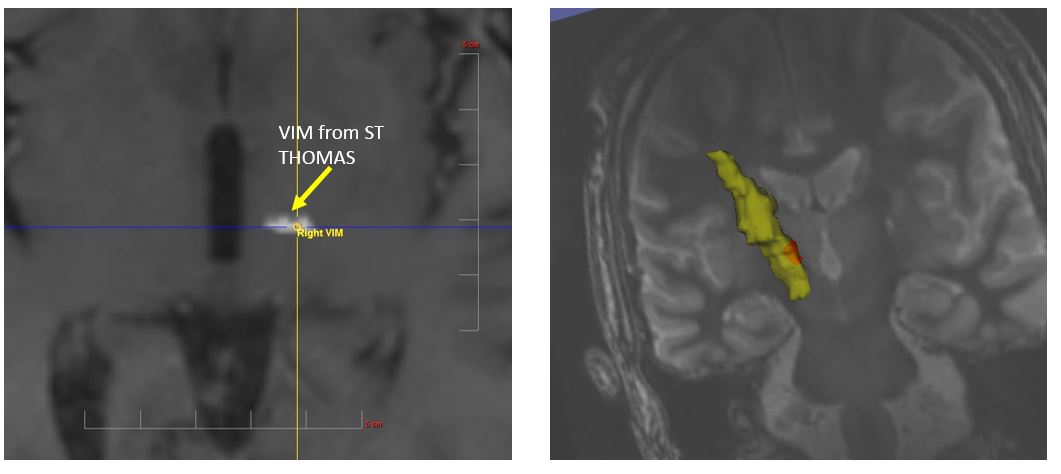
Figure 2 shows the VLP/VIM nucleus segmented from pre-op WMN-MPRAGE using ST THOMAS overlaid on post-op WMN-MPRAGE images on 4 patients. The location of the lead is visible as an artifact on the gradient echo MPRAGE images (assuming successful lead placement) and is clearly overlapping with the VIM nucleus as segmented by ST THOMAS. Figure 3 shows the VLP/VIM nucleus segmented from pre-op WMN-MPRAGE overlaid on post-op Cube T2 images on patient 4. Note the smaller extent of the metal artifacts on the spin-echo Cube images compared to the gradient-echo images in Fig 2. A 3D rendering of the electrode (yellow) and VIM nucleus (red) is also shown (right panel), clearly showing the location of the electrode tip touching the VIM nucleus segmented by ST THOMAS. Figure 4 shows a screen shot from the ClearPoint navigation system on a patient undergoing asleep DBS showing the VIM nucleus from ST THOMAS segmented from pre-op and warped onto an intra-op WMN-MPRAGE scan (yellow arrow) and the target chosen based on atlas coordinates. The right panel shows a 3D rendering of the metal electrode (yellow) and VIM nucleus (red). On this case, the surgeon placed the distal contact point of the electrode beyond the VIM nucleus to enable stimulation of the posterior subthalamic region, clearly visualized.Conclusions
In conclusion, we have shown on patients that WMN-MPRAGE along with ST THOMAS can be used to successfuly segment the VIM nucleus in under ten minutes to enable VIM targeting for asleep DBS. We expect this to be much more accurate than atlas based targeting as it is tailored to individual patients.Acknowledgements
No acknowledgement found.References
1. Tourdias et al. Neuroimage, 84:534-545 (2013)
2. Thomas et al. Proceedings of the ISMRM 2017, p4736
Figures