0689
Multi-vendor validation and reproducibility of 4D flow MRI using 4-fold parallel imaging acceleration with and without respiratory gating1Clinical Physiology, Department of Clinical Sciences, Skane University Hospital, Lund University, Lund, Sweden, 2Department of Biomedical Engineering, Faculty of Engineering, Lund University, Lund, Sweden, 3Lund University Bioimaging Center, Lund University, Lund, Sweden, 4Philips Healthcare, Lund, Sweden, 5Siemens Healthcare AB, Malmö, Sweden, 6Siemens Healthcare GmbH, Erlangen, Germany
Synopsis
4D-flow sequences on two 1.5T scanners from different vendors (Philips Achieva dStream and Siemens MAGNETOM Aera) were validated head-to-head. 4D-flow in a pulsatile flow phantom showed high accuracy and precision compared to reference laser particle image velocimetry for both scanners. 2D-flows in ascending and descending aorta and pulmonary trunk were compared to 57 4D-flow scans in 10 subjects. Lower bias for flow volumes was found on Aera (-4.7±12.5%) compared to Achieva (-18.0±20.1%). Kinetic energy showed lower bias for repeated examinations at the same scanner compared to different scanners the same day. 4D-flow without respiratory gating on Aera showed acceptable quality.
Background
We aimed to validate 4D-flow sequences from two vendors in phantom and in vivo, comparing the results of absolute flow and kinetic energy (KE) head-to-head, with and without respiratory gating.Methods
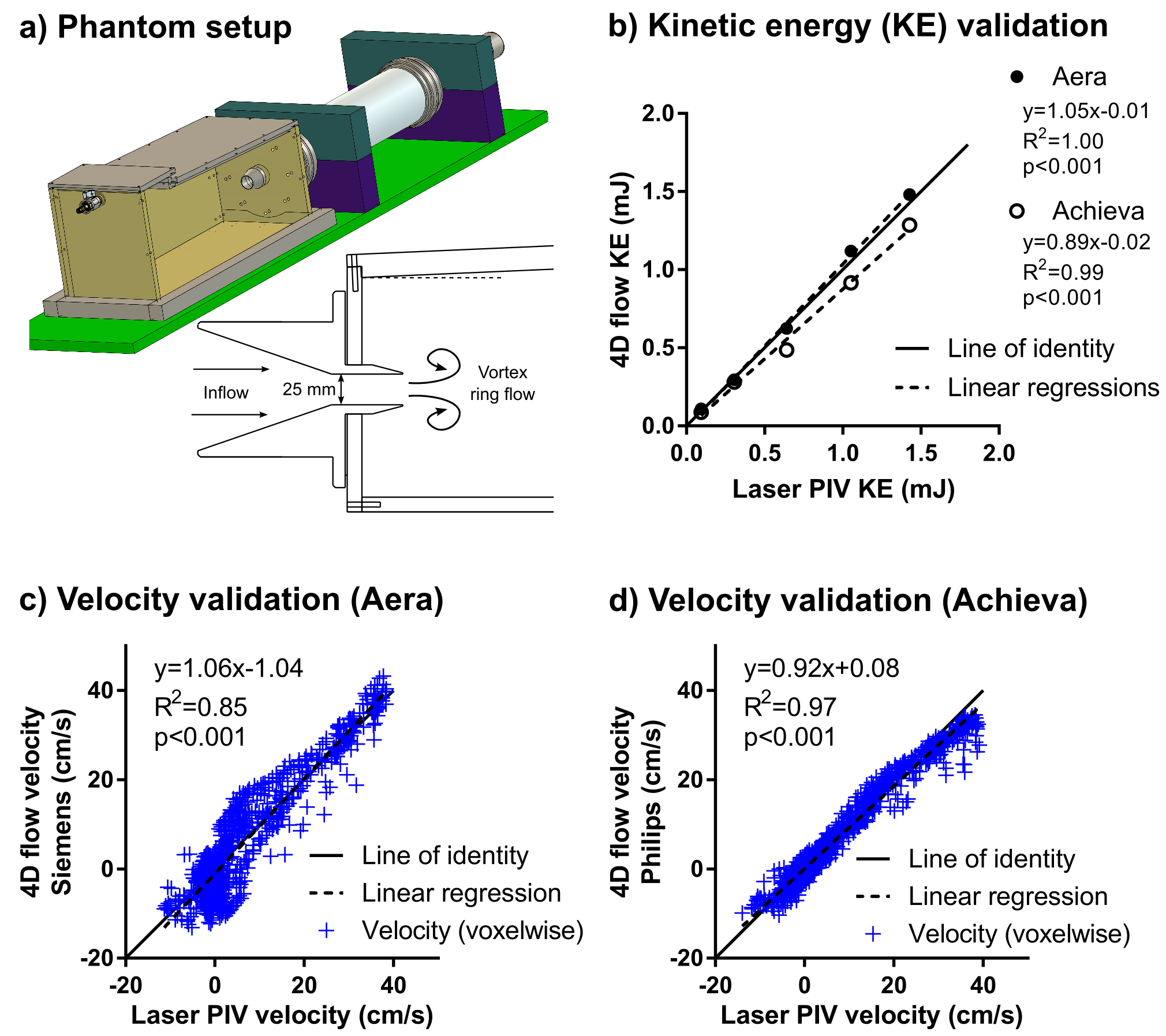
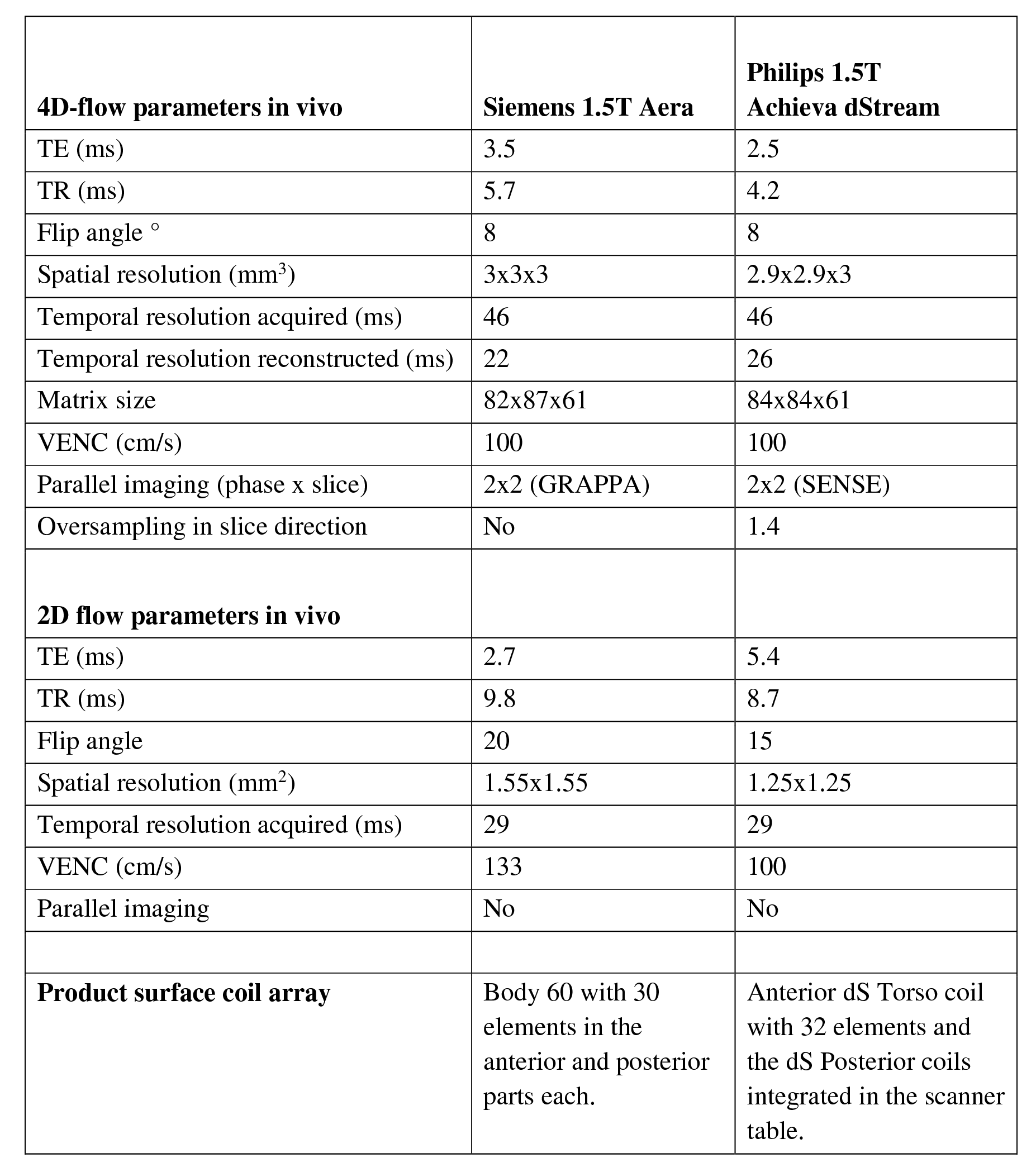
Experiments were performed on an Achieva dStream (Philips Healthcare, Best, The Netherlands) and a MAGNETOM Aera (Siemens Healthcare, Erlangen, Germany) 1.5T scanners. Phantom validation (Figure 1a) was performed using a setup (1) enabling measurement of a pulsatile and fully three-dimensional water flow with 4D-flow MRI and laser particle imaging velocimetry (PIV) as the reference standard. Three cardiac MRI examinations for each of the ten healthy subjects were performed: 2D-cine in long- and short-axis planes, 2D-flow of the aorta and pulmonary artery and 4D-flow using a product and a prototype sequence on Achieva and Aera, respectively. Examinations were performed consecutively on the same day on both scanners with one additional repeated scan within two weeks. Retrospective ECG-triggered 4D-flow with (Resp+) and without (Resp-) respiratory gating were acquired (Figure 2). Images were analysed using custom plug-ins based on Segment (http://segment.heiberg.se) (2).
Image quality in the 4D flow data was scored by two experienced observers, with a score of 0 being near-perfect quality and 3 the worst. Results are presented both for all acquired data and with suboptimal quality scans excluded. Second observer analysis was performed for 66 vessels from 22 4D-flow scans and the same vessels with 2D-flow.
In vivo flow was calculated from the ascending and descending aorta and pulmonary artery from 2D and 4D-flow acquisitions in identical planes. The contours from 2D-flow were transferred to 4D-flow images for stroke volume estimation. KE for all time phases and voxels in the ventricle (as delineated in the cine short-axis stack) were calculated as KE=½mv2, with voxel mass m and velocity v.
Results
For the phantom validation, voxel-wise comparison of velocities between 4D-flow and laser PIV showed a strong correlation and low bias for both scanners (Figure 1 b,c,d). KE showed good agreement compared to laser PIV on Aera and a slight underestimation on Achieva.
In total 57 in vivo 4D-flow scans were acquired. The re-scans were performed 6±3 days after the first examination.
Average 4D-flow scan durations on Aera and Achieva were 9±3 (Resp+) / 6±2 (Resp-) minutes and 17±3 (Resp+) / 10±1 (Resp-) minutes, respectively. Image quality was better on Aera as on Achieva for both Resp+ (0.7±0.6 vs. 2.0±0.7) and Resp- (0.9±0.6 vs. 2.5±0.5) acquisitions. There was no intra-scanner difference in image quality between 4D-flow Resp+ and Resp- acquisitions. On Aera, no 4D-flow acquisitions had suboptimal image quality for analysis, but four Resp+ (31%) and eight Resp- (57%) acquisitions had suboptimal image quality on Achieva.
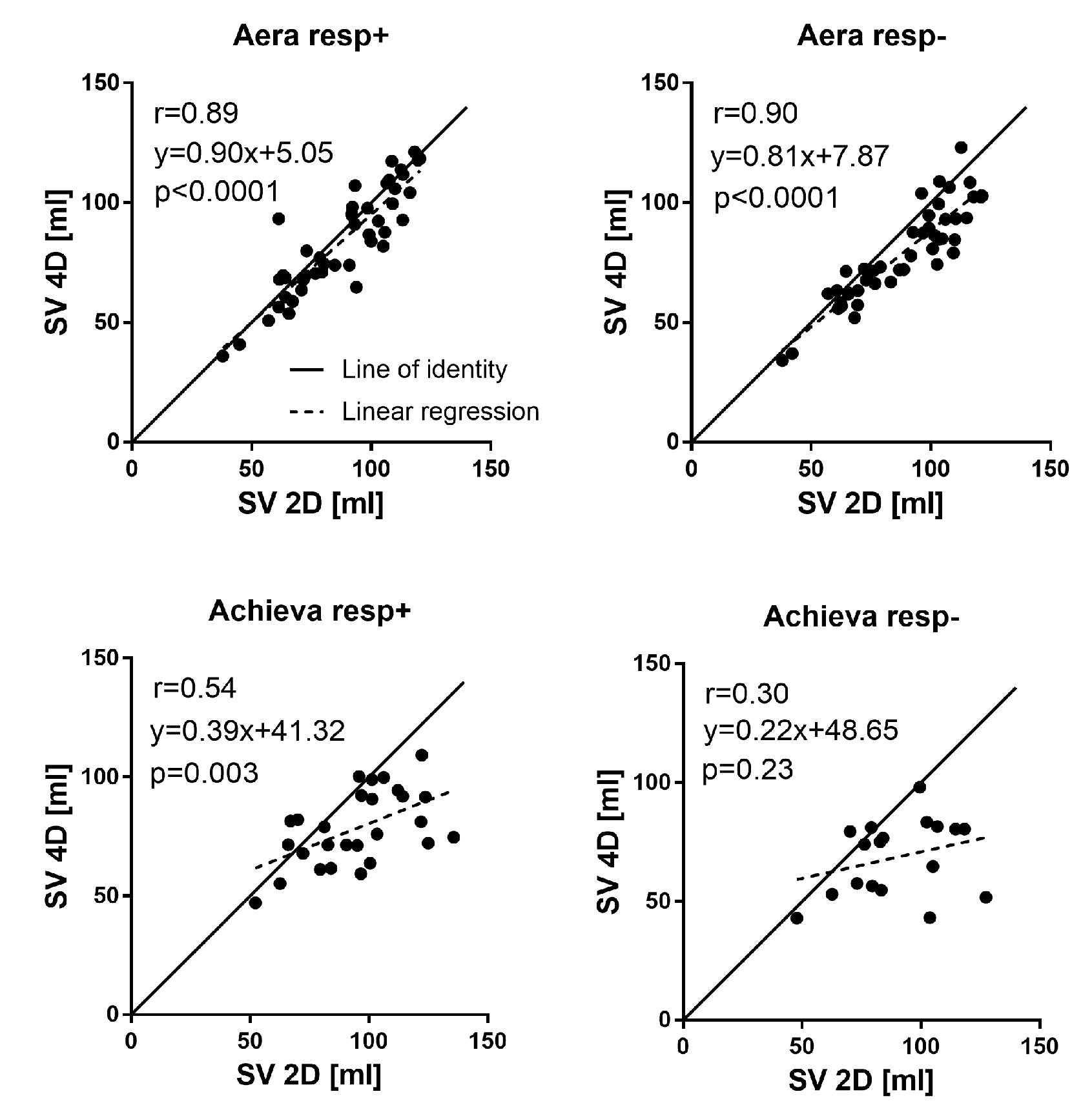
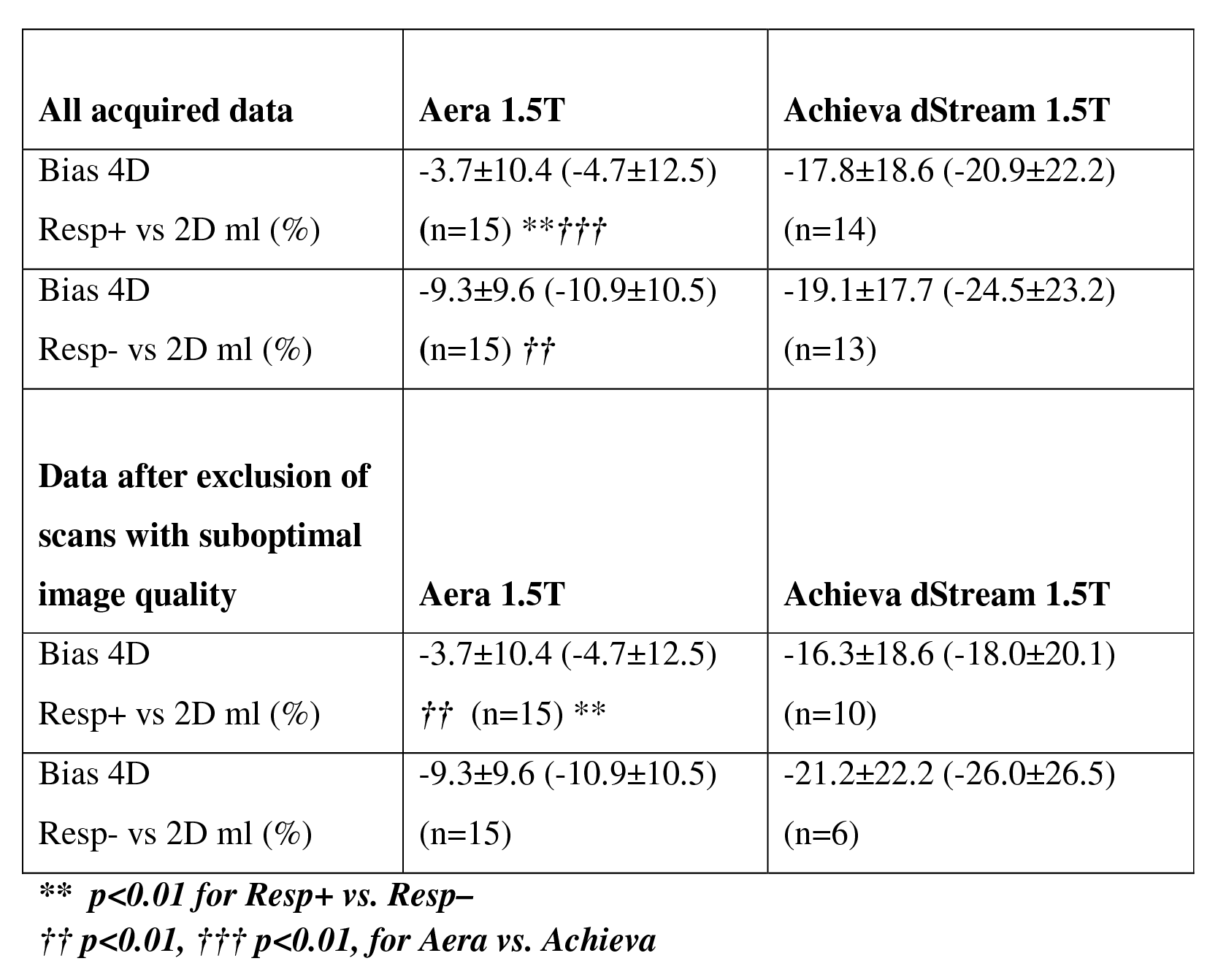
2D-flow before and after 4D-flow acquisitions showed low bias and variability (0.6±8.0 ml). Compared to 2D-flow, 4D-flow underestimated the flow on both scanners (Figures 3 and 4). 4D-flow Resp+ on Aera showed the lowest bias and higher precision, both compared to 4D-flow Resp- (p=0.005) on Aera and 4D-flow Resp+ on Achieva (p<0.001). Bias was not different between 4D-flow Resp+ and Resp- (p=0.87) on Achieva. Excluding acquisitions with suboptimal image quality on Achieva did not improve the bias (Figure 4).
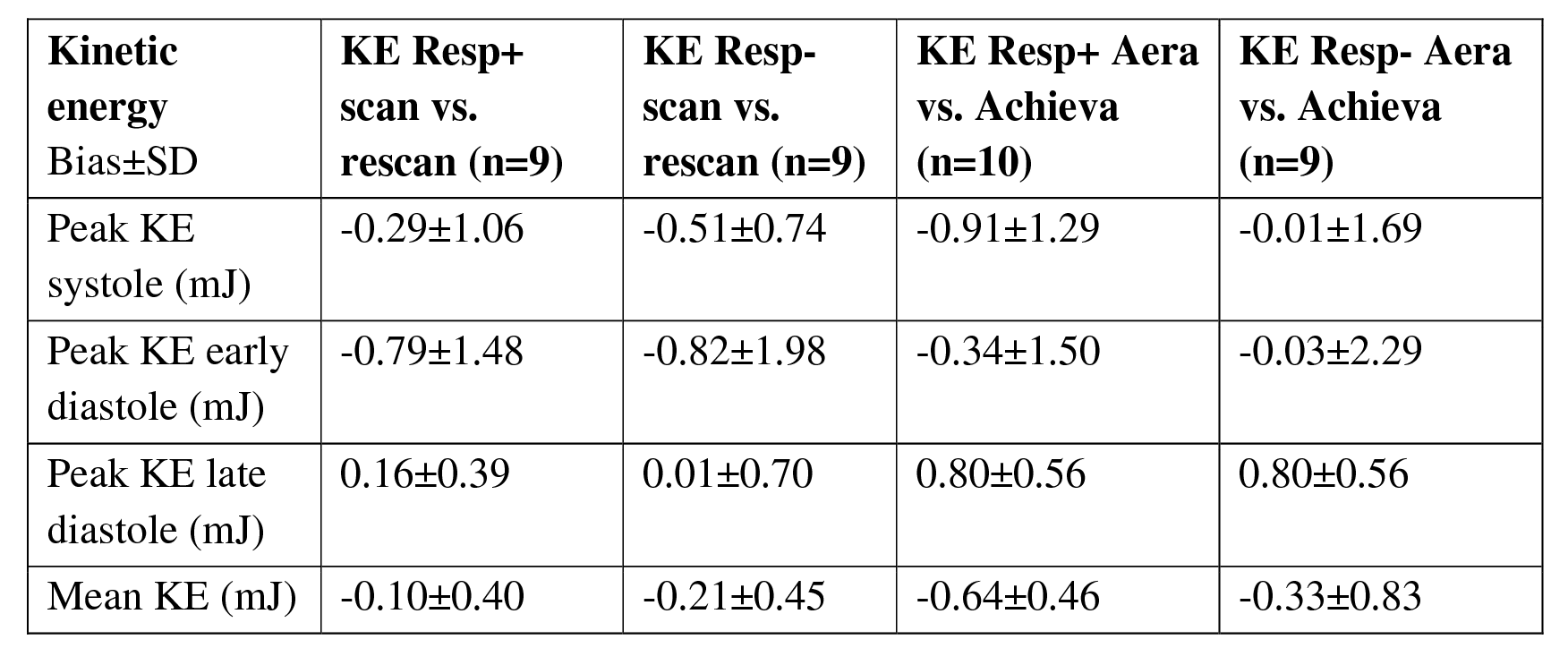
Peak KE in systole and diastole (Figure 5) was similar on Aera (3.9±1.5 and 5.3±1.9 mJ) and Achieva (4.7±1.4 and 5.6±1.6 mJ). Mean KE from 4D-flow was lower on Aera (1.7±0.6 mJ) compared to Achieva (2.3±0.5, p<0.01).
Inter-observer variability for 4D-flow measurements (66 vessels) was 1.3±2.1 ml and for 2D-flow was 0.2±5.9 ml.
Discussion
This is the first study to validate the Siemens prototype compared to Philips 4D-flow sequence head-to-head. Phantom results show high accuracy and precision for both sequences. In vivo, higher accuracy and precision was found for stroke volume for the 4D-flow prototype compared to Philips sequence. The difference in bias may be scanner- rather than vendor-dependent. Longer 4D-flow duration on Achieva was principally due oversampling in the slice direction and lower image quality could be due to sub-optimal image reconstruction in slice direction. Results of 4D-flow Resp- on Siemens demonstrate a further possibility to decrease 4D-flow scan time. KE estimations show differences between scanners that are larger than KE differences from the same scanner over time.Conclusion
The study shows the importance of in vivo validation of 4D-flow for each scanner and sequence before clinical use. 4D-flow of the Siemens prototype sequence may replace 2D-flow with a clinically acceptable acquisition time. Patients followed over time with KE estimation need to be examined using the same scanner.Acknowledgements
No acknowledgement found.References
1. Töger J, Bidhult S, Revstedt J, Carlsson M, Arheden H, Heiberg E: Independent validation of four-dimensional flow MR velocities and vortex ring volume using particle imaging velocimetry and planar laser-Induced fluorescence. Magn Reson Med 2016; 75:1064–1075.
2. Heiberg E, Sjögren J, Ugander M, Carlsson M, Engblom H, Arheden H: Design and validation of Segment - freely available software for cardiovascular image analysis. BMC Med Imaging 2010; 10:1.
Figures