0688
Real-time and self-gated flow using a golden-angle spiral trajectory1Cardiovascular Interventions Program, National Heart, Lung & Blood Institute, Bethesda, DC, United States, 2Biochemistry and Biophysics Center, National Heart, Lung & Blood Institute, Bethesda, DC, United States
Synopsis
Beat-to-beat measurements of cardiac output have been demonstrated as a valuable diagnostic tool during interventional cardiovascular MR procedures with physiological provocations such as exercise. This preliminary study investigates the potential of golden-angle spiral imaging for combined real-time and retrospectively-binned flow measurements at rest and during exercise. In flow phantoms and human subjects, good agreement was observed between reference Cartesian measurements and self-gated spiral acquisitions at rest. During exercise, real-time and self-gated spiral imaging measured an increase in cardiac output, demonstrating this technique’s potential application to interventional MRI.
Introduction
Real-time measurement of cardiac output has been shown to complement interventional cardiovascular MR procedures 1. Beat-to-beat measurements of blood flow can monitor acute response to physiological provocations during diagnostic catheterization, where conventional segmented cardiac imaging, reliant on ECG triggering, is inadequate. We investigate a golden-angle spiral acquisition to measure flow with two analyses: 1) real-time estimation of cardiac output for real-time monitoring and 2) retrospectively self-gated estimation of cardiac output, based on re-binning of beat-to-beat flow data.Methods
Study: Flow phantom (CardioFlow 5000, Shelley Medical, Canada) experiments and n=4 healthy human subject studies were performed at 1.5T (Aera, Siemens Healthcare, Germany). Institutional review board approval and informed consent was obtained for human studies. The flow-phantom was configured to mimic rest and exercise at two heart rates (60 & 90 bpm), and a flow rate of 4.5 L/min. Real-time flow through the ascending aorta was acquired at rest during free breathing, and two of the subjects were imaged during exercise using a MR-compatible ergometer (CardioStep, Ergospect, Austria).
Pulse sequence: An eight-shot spiral design 2 was modified to rotate by the golden angle (typical sequence parameters: TR/TE = 9.2/1.6 ms, 2.7 x 2.7 mm2 resolution, 6 mm slice thickness, typical venc = 150/200 cm/s at rest/exercise). The sequence was acquired for 18 seconds both at rest and exercise.
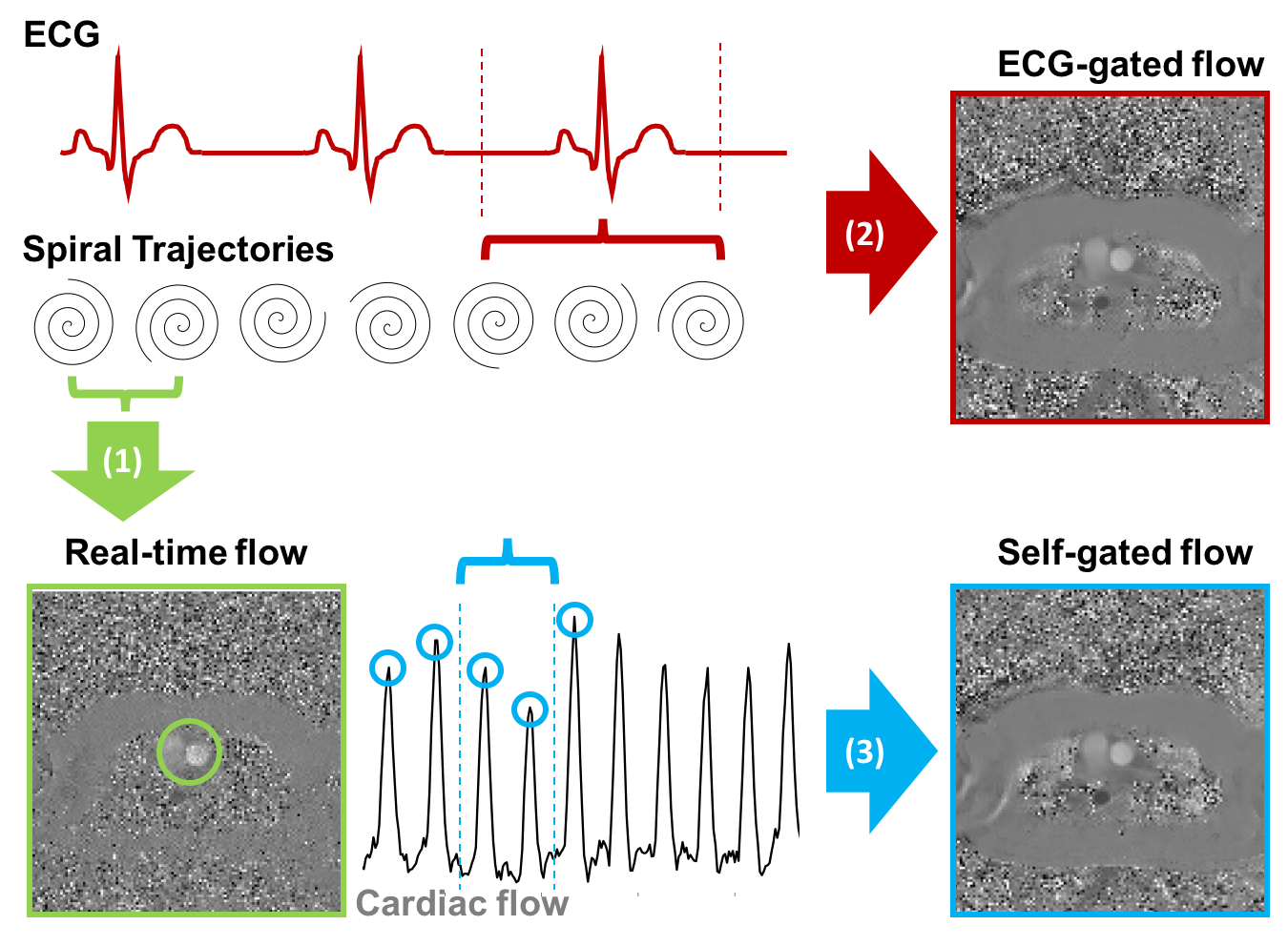
Reconstruction: Golden-angle spiral flow data was reconstructed three ways (fig. 1):
1) as a real-time data stream using successive spiral arms (acceleration factor 4, temporal resolution 36.8 ms) to obtain beat-to-beat cardiac output 3
2) retrospectively binned in to a single cardiac cycle, using the recorded ECG
3) retrospectively binned in to a single cardiac cycle, using the real-time flow data to generate a self-gated image.
Thirty cardiac frames with a temporal resolution of 30.2 ± 6.6 ms for retrospective reconstructions were reconstructed using iterative conjugate gradient SENSE 4 in Matlab (Mathworks, USA).
Quantification: Reference ECG-gated Cartesian flow data was slice- and venc-matched, and acquired with the following parameters: 1.4 x 1.4 mm2 resolution, TE/TR = 2.8/5.0 ms, 3 averages, acceleration factor 3 in human subjects at rest and stress. For both spiral and Cartesian imaging, a single region-of-interest was manually drawn and used for flow quantification.
Results
Flow phantom: There was no significant difference between the cardiac output estimated by the three golden-angle spiral reconstructions (Friedman test p > 0.07), however, these significantly under-estimated cardiac output (Friedman test p < 0.002) in comparison to equivalent Cartesian data. Average real-time, ECG-binned, and self-gated-binned relative cardiac output were respectively 95 ± 4%, 94 ± 4%, and 95± 4% relative to Cartesian data.
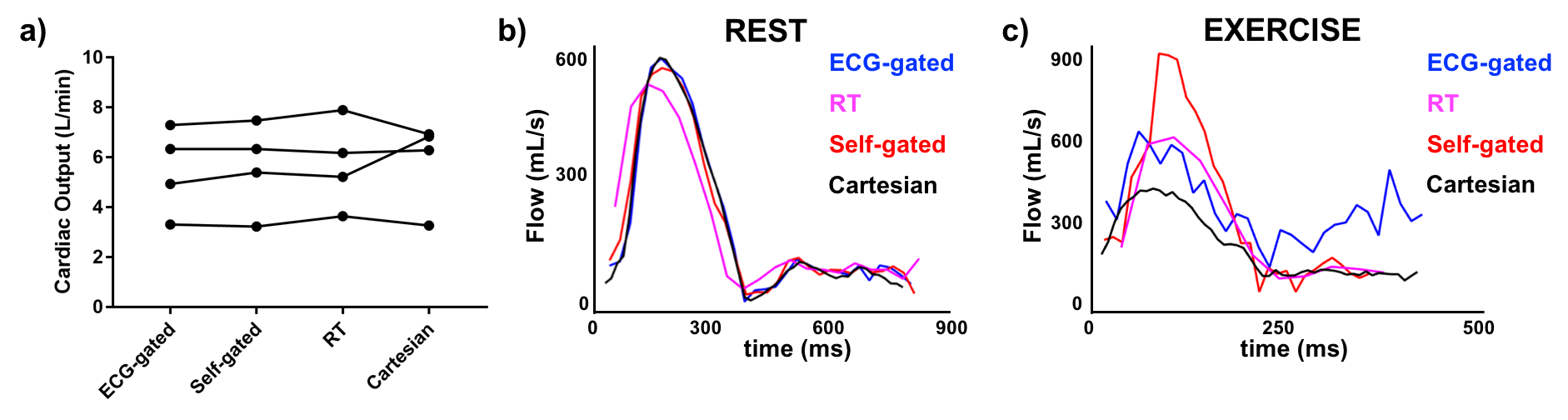
Human subjects: there was no significant difference between cardiac output at rest as measured by the reference Cartesian acquisition and any of the three techniques (fig. 2a & b, fig. 3) (Friedman test p > 0.9). Relative cardiac output measured by real-time, ECG-binned, self-gated reconstruction was respectively 100 ± 15%, 95 ± 13%, 97 ± 11% compared to the Cartesian reference (mean ± std., 5.8 ± 1.5 L/min, n = 4). During exercise, the increase in cardiac output was measured with real-time imaging (5.7± 0.7 to 9.6 ± 0.7 L/min) and self-gated data (5.9± 0.7 to 13.0 ± 1.8 L/min). The self-gated and real-time data preserved the expected flow profile, where the ECG-gated reconstructions yielded signal artifacts (fig. 2c) due to the motion-corrupted ECG signal.
Discussion and Conclusion
In this preliminary study, we have implemented a real-time flow sequence employing a golden angle sampling pattern that enables both a beat-to-beat and self-gated binned velocity encoded image data from a single data stream. Self-gating produced comparable images to ECG-binned data at rest, and demonstrated it is viable during exercise physiological provocation, where the ECG-gated fails. The discrepancy between spiral and Cartesian flow values in the phantom is potentially due to both partial-volume effects at the lower resolution, and image artifacts caused by apparatus set-up.
Finally, we envisage this technique can contribute to MRI-guided cardiovascular intervention by enabling real-time monitoring of provocations combined with retrospectively-gated datasets for improved quantification.
Acknowledgements
This work was supported by the NHLBI DIR (Z01-HL006039, Z01-HL005062).References
[1] Barber NJ, Ako EO, Kowalik GT, Steeden JA, Pandya B, and Muthurangu V. MR augmented cardiopulmonary exercise testing-a novel approach to assessing cardiovascular function. Physiol. Meas., 2015; 36: N85-94.
[2] Lee JH, Hargreaves BA, Hu BS, and Nishimura DG. Fast 3D imaging using variable-density spiral trajectories with applications to limb perfusion. Magn. Reson. Med., 2003; 50: 1276–1285. doi:10.1002/mrm.10644.
[3] Ramasawmy R, Faranesh AZ, Khan JM, Rogers T, Lederman RJ, Hansen MS, and Campbell-Washburn AE. Real-time monitoring of Exercise Stress using Spiral Flow MRI. ISMRM 2017; 2841.
[4] Pruessmann KP, Weiger M, Bornert P, and Boesiger P. Advances in sensitivity encoding with arbitrary k-space trajectories. Magn. Reson. Med., 2001; 46: 638-51.
Figures