0686
Inefficient Right Heart Function in Preterm Adults as shown with 4D Flow MRI1Medical Physics, University of Wisconsin - Madison, Madison, WI, United States, 2Pediatrics, University of Wisconsin - Madison, Madison, WI, United States, 3Radiology, University of Wisconsin - Madison, Madison, WI, United States
Synopsis
Infants born preterm often have impaired pulmonary function, but little is known regarding long-term implications on right-heart function as these patients reach adulthood. We performed 4D flow MRI during rest and exercise in young adults born preterm and age-matched controls to compare their right heart function and efficiency. While flow and velocity in the pulmonary artery appeared similar in both groups, preterm subjects demonstrated increased kinetic energy in the right ventricle (RV) per unit of ejected blood. Pathline visualizations in the right ventricle suggested less structured filling during diastole. These data suggests decreased RV efficiency in preterm adults.
Introduction
Improved preterm-birth survival in the past few decades has led to a new patient population with unique health challenges. While the short-term impacts of preterm-birth have been well-described1, the long-term consequences are not well understood due to previously poor survival rates in this group. A recent MRI study showed reduced right ventricle (RV) volumes and greater RV mass in preterm-birth adults2. This notable RV dysfunction may indicate an increased risk of cardiovascular disease as this patient population ages. As a result, biomarkers for understanding the underlying mechanisms, as well as early diagnosis and management, will be needed. Here, we investigated using an MRI exercise challenge and 4D flow MRI for additional comparisons of right heart efficiency in preterm adults and controls.Methods
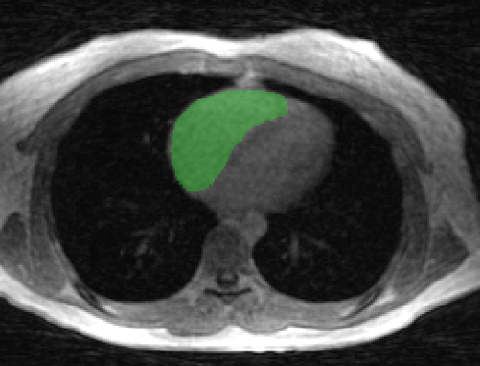
Twenty-two subjects were imaged on a clinical 3.0T scanner (Discovery 750, GE Healthcare) with an 8-channel cardiac coil: 11 preterm-birth adults (27±1 years; 5 male, 6 female) and 11 normal-birth controls (26±1 years; 8 male, 3 female). 4D flow imaging at rest and during exercise was performed with a radially-undersampled PC VIPR3,4 sequence (TR/TE=6.2/2.0ms; FA=10°; VENC=200cm/s; FOV=32x32x32cm; acquired spatial resolution=1.25mm isotropic; scan time=9.25 min) with retrospective respiratory and ECG gating (15 cardiac phases). Exercise was conducted in the magnet bore with an MR-compatible exercise stepper (Ergospect GmbH) at 70% of each subject’s VO2,max. Flow and velocity measurements were performed in the main pulmonary artery (MPA) using a customized MATLAB tool5. To assess RV kinetic energy (KE), the RV was segmented from time-averaged PC VIPR magnitude images in Mimics (Materialize) (Figure 1). This mask was applied to the time-resolved velocity images, and the KE in the RV across the cardiac cycle was computed using the formula below. $$KE_{total}=\sum\limits_1^{frames}\sum\limits_1^{voxels}\frac{1}{2}mv^2_{mag}$$ To characterize energy efficiency in the RV, the total KE across the cardiac cycle was normalized by the stroke volume6. For all parameters, statistical significance (p<0.05) was assessed with t-tests.
Results
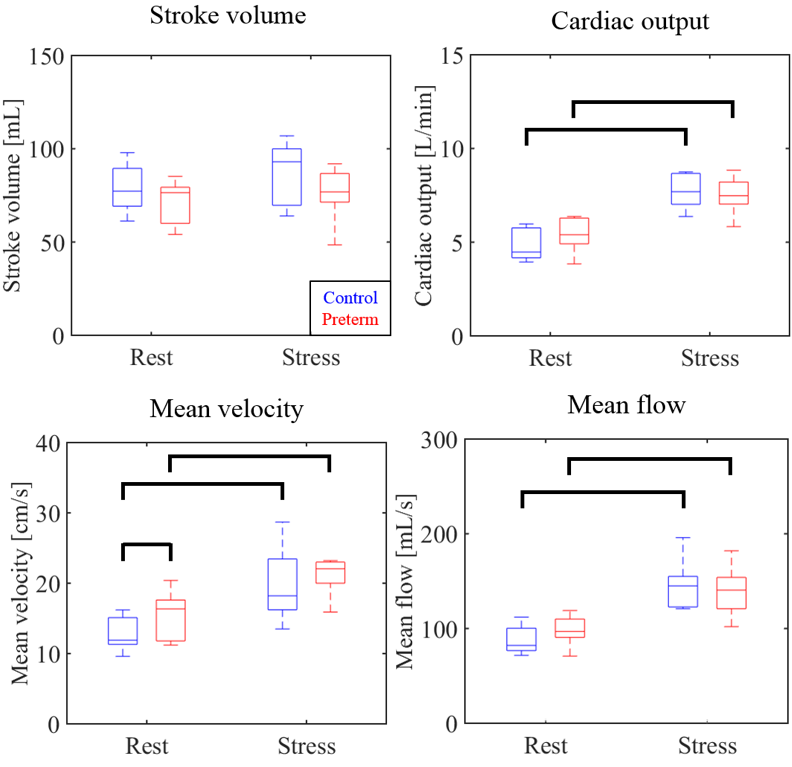
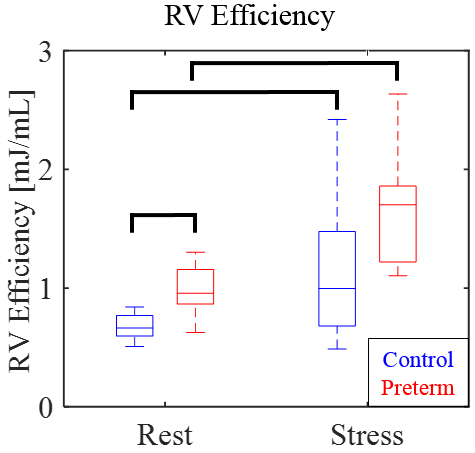
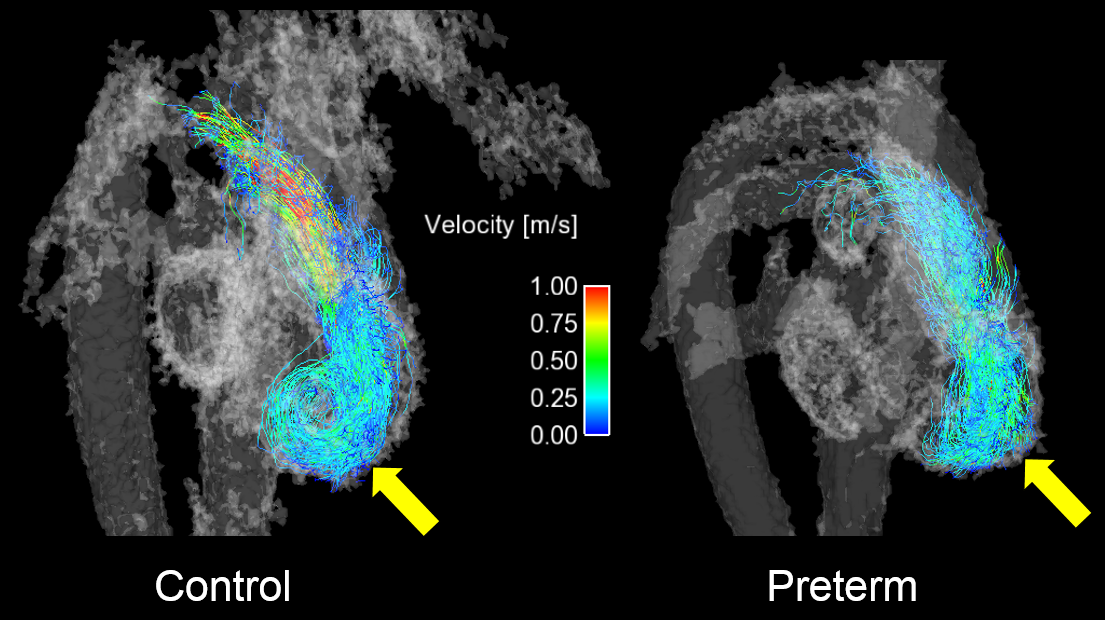
Control subjects demonstrated an average increase in heart rate of 44% with exercise, while preterm subjects showed a 40% increase. Cardiac output, mean velocity, and mean flow showed statistically significant increases with exercise for both groups, but with the exception of mean velocity at rest, there were no significant intergroup differences at either rest or stress (Figure 2). While stroke volume showed no significant differences at rest or stress, control group stroke volume trended toward an increase with exercise (p=0.08) while the preterm group did not (p=0.34). The preterm cohort demonstrated a decreased stroke volume distribution at rest, consistent with the findings of Lewandowski et al2. KE normalized by stroke volume proved to be sensitive to intergroup differences (Figure 3). Pathline comparisons of preterm subjects and controls with similar stroke volumes showed less structure to the flow vortex present during ventricular filling in the preterm subjects (Figure 4).Discussion
For cardiac output, mean velocity, and mean flow, there were no significant differences between the preterm subjects and controls. This was not unexpected, as the inclusion criteria of preterm subjects were biased towards healthy preterm adults who could endure a graded exercise stress test. Notably, the preterm subjects did not all demonstrate similar increases in stroke volume during exercise, suggesting a greater reliance on increasing heart rate to raise cardiac output. The preterm subjects demonstrated significantly increased KE per milliliter of blood ejected during the cardiac cycle. This finding suggests an underlying inefficiency in their RV function relative to the healthy controls. Pathline analysis suggested that this inefficiency may be linked to less coherent filling of the RV. This is consistent with previous work that has hypothesized that a filling vortex helps dissipate excessive KE that would otherwise increase ventricular pressure and impede inflow7. A reduction in the efficiency of these vortices in preterm subjects, as witnessed here, would require the heart to work harder for an equivalent stroke volume compared to a healthy subject.Conclusion
In this study, we introduced an exercise challenge and 4D flow MRI to investigate if preterm birth had any long-term impacts on right-heart function. While parameters such as cardiac output, mean flow, and mean velocity suggested similar cardiac performance between preterms and controls, increased total RV KE normalized by stroke volume suggested a decreased right heart efficiency in the preterm cohort. From qualitative pathline comparisons in patients and controls with similar stroke volumes, we hypothesize that this inefficiency may be linked to less prominent ventricular filling vortices in these subjects. These signs of increased cardiac workload in otherwise healthy preterm adults are concerning and warrant future work investigating relationships to the cardiac health of these subjects.Acknowledgements
We gratefully acknowledge funding from the NIH (R01 HL086897, R01 HL38149) and research support from GE Healthcare.References
1. Bhatt AJ, Pryhuber GS, Huyck H, Watkins RH, et al. Disrupted pulmonary vasculature and decreased vascular endothelial growth factor, Flt-1, and TIE-2 in human infants dying with bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001; 164(10):1971-1980.
2. Lewandowski AJ, Bradlow WM, Augustine D, Davis EF, et al. Right Ventricular Systolic Dysfunction in Young Adults Born Preterm. Circulation. 2013; 128(7): 713-720.
3. Gu T, Korosec FR, Block WF, Fain SB, et al. PC VIPR: a high-speed 3D phase-contrast method for flow quantification and high-resolution angiography. AJNR. 2005; 26(4): 743-749.
4. Johnson KM, Lum DP, Turski PA, Block WF, et al. Improved 3D phase contrast MRI with off-resonance corrected dual echo VIPR. MRM. 2008;60(6):1329-1336.
5. Stalder AF, Russe MF, Frydrychowicz A, Bock J, et al. Quantitative 2D and 3D phase contrast MRI: Optimized analysis of blood flow and vessel wall parameters. MRM. 2008; 60(5): 1218-1231.
6. Jeong D, Anagnostopoulos PV, Roldan-Alzate A, Srinivasan S, et al. Ventricular kinetic energy may provide a novel noninvasive way to assess ventricular performance in patients with repaired tetralogy of Fallot. 2015; 149(5): 1339-1347.
7. Pasipoularides A, Shu M, Shah A, Womack MS, Glower DD. Diastolic right ventricular filling vortex in normal and volume overload states. Am J Physiol Heart Circ Physiol. 2003; 284: 1064-1072.
Figures